Health and Education: the Importance of Health Education
This essay about the interplay between health and education discusses how health education acts as a vital component in human development. It highlights the role of health education in empowering individuals and communities to make informed health choices, emphasizing its impact on both physical and mental well-being. The essay also explores how health education can inspire societal change through advocacy and community engagement, ultimately aiming for a healthier, more equitable world.
How it works
In the intricate choreography of well-being and enlightenment, the synergy between health and education intertwines, each harmonizing with the other to orchestrate a symphony of human development. Within this dynamic interplay lies the essence of health education—a guiding beacon steering individuals and societies towards a luminous, healthier future.
In the vivid mosaic of health education, myriad shades emerge, creating a canvas of empowerment, prevention, and advocacy. At its nucleus, health education serves as a compass navigating individuals through the labyrinth of wellness, equipping them with the knowledge and resources to make enlightened decisions about their health.
Picture a community where health education reigns supreme, its influence permeating every nook and cranny, from bustling urban hubs to secluded rural hamlets. Here, awareness blossoms like a kaleidoscope of flowers in springtime, as individuals embrace preventive measures and cultivate healthy habits as innate as breathing.
Contemplate the ripple effect of health education on disease prevention—a cascade of awareness that shatters the shackles of illness and suffering. Through targeted campaigns and grassroots endeavors, communities arm themselves with the shield of information, thwarting infectious diseases and chronic ailments alike.
However, the tapestry of health education extends beyond physical well-being alone; its brushstrokes delve into the realm of mental health, dispelling the shadows of stigma and ignorance. Within these strokes lies the promise of destigmatization, fostering open dialogues and fostering empathetic understanding that nurture resilient minds and compassionate hearts.
In the realm of education, health education assumes center stage, infusing curricula with the essence of well-being and self-care. Here, students embark on a voyage of self-discovery, learning not only academic subjects but also the art of resilience, the science of nutrition, and the importance of seeking support when necessary.
Yet, health education transcends the confines of textbooks; it is a philosophy that permeates every facet of life, shaping attitudes and behaviors towards a healthier, more equitable society. Through community engagement and policy advocacy, health educators become catalysts for change, spearheading initiatives that dismantle barriers to wellness and champion health equity for all.
In the grand tapestry of global health, health education emerges as a guiding light in times of crisis. Amidst the tumult of pandemics and emergencies, it stands firm, disseminating accurate information, dispelling misinformation, and galvanizing communities into action.
Ultimately, the significance of health education transcends borders, weaving a common thread that binds us all in our shared pursuit of well-being. As we navigate the vast expanse of human existence, let us remember that the odyssey to health and enlightenment commences with a single step—a step guided by the beacon of knowledge and fueled by the passion to cultivate a healthier, happier world for generations to come.

Cite this page
Health And Education: The Importance Of Health Education. (2024, Apr 29). Retrieved from https://papersowl.com/examples/health-and-education-the-importance-of-health-education/
"Health And Education: The Importance Of Health Education." PapersOwl.com , 29 Apr 2024, https://papersowl.com/examples/health-and-education-the-importance-of-health-education/
PapersOwl.com. (2024). Health And Education: The Importance Of Health Education . [Online]. Available at: https://papersowl.com/examples/health-and-education-the-importance-of-health-education/ [Accessed: 25 Sep. 2024]
"Health And Education: The Importance Of Health Education." PapersOwl.com, Apr 29, 2024. Accessed September 25, 2024. https://papersowl.com/examples/health-and-education-the-importance-of-health-education/
"Health And Education: The Importance Of Health Education," PapersOwl.com , 29-Apr-2024. [Online]. Available: https://papersowl.com/examples/health-and-education-the-importance-of-health-education/. [Accessed: 25-Sep-2024]
PapersOwl.com. (2024). Health And Education: The Importance Of Health Education . [Online]. Available at: https://papersowl.com/examples/health-and-education-the-importance-of-health-education/ [Accessed: 25-Sep-2024]
Don't let plagiarism ruin your grade
Hire a writer to get a unique paper crafted to your needs.

Our writers will help you fix any mistakes and get an A+!
Please check your inbox.
You can order an original essay written according to your instructions.
Trusted by over 1 million students worldwide
1. Tell Us Your Requirements
2. Pick your perfect writer
3. Get Your Paper and Pay
Hi! I'm Amy, your personal assistant!
Don't know where to start? Give me your paper requirements and I connect you to an academic expert.
short deadlines
100% Plagiarism-Free
Certified writers
- Open access
- Published: 06 April 2020
The influence of education on health: an empirical assessment of OECD countries for the period 1995–2015
- Viju Raghupathi 1 &
- Wullianallur Raghupathi 2
Archives of Public Health volume 78 , Article number: 20 ( 2020 ) Cite this article
230k Accesses
320 Citations
176 Altmetric
Metrics details
A clear understanding of the macro-level contexts in which education impacts health is integral to improving national health administration and policy. In this research, we use a visual analytic approach to explore the association between education and health over a 20-year period for countries around the world.
Using empirical data from the OECD and the World Bank for 26 OECD countries for the years 1995–2015, we identify patterns/associations between education and health indicators. By incorporating pre- and post-educational attainment indicators, we highlight the dual role of education as both a driver of opportunity as well as of inequality.
Adults with higher educational attainment have better health and lifespans compared to their less-educated peers. We highlight that tertiary education, particularly, is critical in influencing infant mortality, life expectancy, child vaccination, and enrollment rates. In addition, an economy needs to consider potential years of life lost (premature mortality) as a measure of health quality.
Conclusions
We bring to light the health disparities across countries and suggest implications for governments to target educational interventions that can reduce inequalities and improve health. Our country-level findings on NEET (Not in Employment, Education or Training) rates offer implications for economies to address a broad array of vulnerabilities ranging from unemployment, school life expectancy, and labor market discouragement. The health effects of education are at the grass roots-creating better overall self-awareness on personal health and making healthcare more accessible.
Peer Review reports
Introduction
Is education generally associated with good health? There is a growing body of research that has been exploring the influence of education on health. Even in highly developed countries like the United States, it has been observed that adults with lower educational attainment suffer from poor health when compared to other populations [ 36 ]. This pattern is attributed to the large health inequalities brought about by education. A clear understanding of the health benefits of education can therefore serve as the key to reducing health disparities and improving the well-being of future populations. Despite the growing attention, research in the education–health area does not offer definitive answers to some critical questions. Part of the reason is the fact that the two phenomena are interlinked through life spans within and across generations of populations [ 36 ], thereby involving a larger social context within which the association is embedded. To some extent, research has also not considered the variances in the education–health relationship through the course of life or across birth cohorts [ 20 ], or if there is causality in the same. There is therefore a growing need for new directions in education–health research.
The avenues through which education affects health are complex and interwoven. For one, at the very outset, the distribution and content of education changes over time [ 20 ]. Second, the relationship between the mediators and health may change over time, as healthcare becomes more expensive and/or industries become either more, or less hazardous. Third, some research has documented that even relative changes in socioeconomic status (SES) can affect health, and thus changes in the distribution of education implies potential changes in the relationship between education and health. The relative index of inequality summarizes the magnitude of SES as a source of inequalities in health [ 11 , 21 , 27 , 29 ]. Fourth, changes in the distribution of health and mortality imply that the paths to poor health may have changed, thereby affecting the association with education.
Research has proposed that the relationship between education and health is attributable to three general classes of mediators: economic; social, psychological, and interpersonal; and behavioral health [ 31 ]. Economic variables such as income and occupation mediate the relationship between education and health by controlling and determining access to acute and preventive medical care [ 1 , 2 , 19 ]. Social, psychological, and interpersonal resources allow people with different levels of education to access coping resources and strategies [ 10 , 34 ], social support [ 5 , 22 ], and problem-solving and cognitive abilities to handle ill-health consequences such as stress [ 16 ]. Healthy behaviors enable educated individuals to recognize symptoms of ill health in a timely manner and seek appropriate medical help [ 14 , 35 ].
While the positive association between education and health has been established, the explanations for this association are not [ 31 ]. People who are well educated experience better health as reflected in the high levels of self-reported health and low levels of morbidity, mortality, and disability. By extension, low educational attainment is associated with self-reported poor health, shorter life expectancy, and shorter survival when sick. Prior research has suggested that the association between education and health is a complicated one, with a range of potential indicators that include (but are not limited to) interrelationships between demographic and family background indicators [ 8 ] - effects of poor health in childhood, greater resources associated with higher levels of education, appreciation of good health behaviors, and access to social networks. Some evidence suggests that education is strongly linked to health determinants such as preventative care [ 9 ]. Education helps promote and sustain healthy lifestyles and positive choices, nurture relationships, and enhance personal, family, and community well-being. However, there are some adverse effects of education too [ 9 ]. Education may result in increased attention to preventive care, which, though beneficial in the long term, raises healthcare costs in the short term. Some studies have found a positive association between education and some forms of illicit drug and alcohol use. Finally, although education is said to be effective for depression, it has been found to have much less substantial impact in general happiness or well-being [ 9 ].
On a universal scale, it has been accepted that several social factors outside the realm of healthcare influence the health outcomes [ 37 ]. The differences in morbidity, mortality and risk factors in research, conducted within and between countries, are impacted by the characteristics of the physical and social environment, and the structural policies that shape them [ 37 ]. Among the developed countries, the United States reflects huge disparities in educational status over the last few decades [ 15 , 24 ]. Life expectancy, while increasing for all others, has decreased among white Americans without a high school diploma - particularly women [ 25 , 26 , 32 ]. The sources of inequality in educational opportunities for American youth include the neighborhood they live in, the color of their skin, the schools they attend, and the financial resources of their families. In addition, the adverse trends in mortality and morbidity brought on by opioids resulting in suicides and overdoses (referred to as deaths of despair) exacerbated the disparities [ 21 ]. Collectively, these trends have brought about large economic and social inequalities in society such that the people with more education are likely to have more health literacy, live longer, experience better health outcomes, practice health promoting behaviors, and obtain timely health checkups [ 21 , 17 ].
Education enables people to develop a broad range of skills and traits (including cognitive and problem-solving abilities, learned effectiveness, and personal control) that predispose them towards improved health outcomes [ 23 ], ultimately contributing to human capital. Over the years, education has paved the way for a country’s financial security, stable employment, and social success [ 3 ]. Countries that adopt policies for the improvement of education also reap the benefits of healthy behavior such as reducing the population rates of smoking and obesity. Reducing health disparities and improving citizen health can be accomplished only through a thorough understanding of the health benefits conferred by education.
There is an iterative relationship between education and health. While poor education is associated with poor health due to income, resources, healthy behaviors, healthy neighborhood, and other socioeconomic factors, poor health, in turn, is associated with educational setbacks and interference with schooling through difficulties with learning disabilities, absenteeism, or cognitive disorders [ 30 ]. Education is therefore considered an important social determinant of health. The influence of national education on health works through a variety of mechanisms. Generally, education shows a relationship with self-rated health, and thus those with the highest education may have the best health [ 30 ]. Also, health-risk behaviors seem to be reduced by higher expenditure into the publicly funded education system [ 18 ], and those with good education are likely to have better knowledge of diseases [ 33 ]. In general, the education–health gradients for individuals have been growing over time [ 38 ].
To inform future education and health policies effectively, one needs to observe and analyze the opportunities that education generates during the early life span of individuals. This necessitates the adoption of some fundamental premises in research. Research must go beyond pure educational attainment and consider the associated effects preceding and succeeding such attainment. Research should consider the variations brought about by the education–health association across place and time, including the drivers that influence such variations [ 36 ].
In the current research, we analyze the association between education and health indicators for various countries using empirical data from reliable sources such as the Organization for Economic Cooperation and Development (OECD) and World Bank. While many studies explore the relationship between education and health at a conceptual level, we deploy an empirical approach in investigating the patterns and relationships between the two sets of indicators. In addition, for the educational indicators, we not only incorporate the level of educational attainment, but also look at the potential socioeconomic benefits, such as enrollment rates (in each sector of educational level) and school life expectancy (at each educational level). We investigate the influences of educational indicators on national health indicators of infant mortality, child vaccinations, life expectancy at birth, premature mortality arising from lack of educational attainment, employment and training, and the level of national health expenditure. Our research question is:
What are some key influencers/drivers in the education-health relationship at a country level?
The current study is important because policy makers have an increasing concern on national health issues and on policies that support it. The effect of education is at the root level—creating better overall self-awareness on personal health and making healthcare more accessible. The paper is organized as follows: Section 2 discusses the background for the research. Section 3 discusses the research method; Section 4 offers the analysis and results; Section 5 provides a synthesis of the results and offers an integrated discussion; Section 6 contains the scope and limitations of the research; Section 7 offers conclusions with implications and directions for future research.
Research has traditionally drawn from three broad theoretical perspectives in conceptualizing the relationship between education and health. The majority of research over the past two decades has been grounded in the Fundamental Cause Theory (FCT) [ 28 ], which posits that factors such as education are fundamental social causes of health inequalities because they determine access to resources (such as income, safe neighborhoods, or healthier lifestyles) that can assist in protecting or enhancing health [ 36 ]. Some of the key social resources that contribute to socioeconomic status include education (knowledge), money, power, prestige, and social connections. As some of these undergo change, they will be associated with differentials in the health status of the population [ 12 ].
Education has also been conceptualized using the Human Capital Theory (HCT) that views it as a return on investment in the form of increased productivity [ 4 ]. Education improves knowledge, skills, reasoning, effectiveness, and a broad range of other abilities that can be applied to improving health. The third approach - the signaling or credentialing perspective [ 6 ] - is adopted to address the large discontinuities in health at 12 and 16 years of schooling, which are typically associated with the receipt of a high school diploma and a college degree, respectively. This perspective considers the earned credentials of a person as a potential source that warrants social and economic returns. All these theoretical perspectives postulate a strong association between education and health and identify mechanisms through which education influences health. While the HCT proposes the mechanisms as embodied skills and abilities, FCT emphasizes the dynamism and flexibility of mechanisms, and the credentialing perspective proposes educational attainment through social responses. It needs to be stated, however, that all these approaches focus on education solely in terms of attainment, without emphasizing other institutional factors such as quality or type of education that may independently influence health. Additionally, while these approaches highlight the individual factors (individual attainment, attainment effects, and mechanisms), they do not give much emphasis to the social context in which education and health processes are embedded.
In the current research while we acknowledge the tenets of these theoretical perspectives, we incorporate the social mechanisms in education such as level of education, skills and abilities brought about by enrollment, school life expectancy, and the potential loss brought about by premature mortality. In this manner, we highlight the relevance of the social context in which the education and health domains are situated. We also study the dynamism of the mechanisms over countries and over time and incorporate the influences that precede and succeed educational attainment.
We analyze country level education and health data from the OECD and World Bank for a period of 21 years (1995–2015). Our variables include the education indicators of adult education level; enrollment rates at various educational levels; NEET (Not in Employment, Education or Training) rates; school life expectancy; and the health indicators of infant mortality, child vaccination rates, deaths from cancer, life expectancy at birth, potential years of life lost and smoking rates (Table 1 ). The data was processed using the tools of Tableau for visualization, and SAS for correlation and descriptive statistics. Approaches for analysis include ranking, association, and data visualization of the health and education data.
Analyses and results
In this section we identify and analyze patterns and associations between education and health indicators and discuss the results. Since countries vary in population sizes and other criteria, we use the estimated averages in all our analyses.
Comparison of health outcomes for countries by GDP per capita
We first analyzed to see if our data reflected the expectation that countries with higher GDP per capita have better health status (Fig. 1 ). We compared the average life expectancy at birth, average infant mortality, average deaths from cancer and average potential year of life lost, for different levels of GDP per capita (Fig. 1 ).

Associations between Average Life Expectancy (years) and Average Infant Mortality rate (per 1000), and between Deaths from Cancer (rates per 100,000) and Average Potential Years of Life Lost (years), by GDP per capita (for all countries for years 1995–2015)
Figure 1 depicts two charts with the estimated averages of variables for all countries in the sample. The X-axis of the first chart depicts average infant mortality rate (per 1000), while that of the second chart depicts average potential years of life lost (years). The Y-axis for both charts depicts the GDP per capita shown in intervals of 10 K ranging from 0 K–110 K (US Dollars). The analysis is shown as an average for all the countries in the sample and for all the years (1995–2015). As seen in Fig. 1 , countries with lower GDP per capita have higher infant mortality rate and increased potential year of life lost (which represents the average years a person would have lived if he or she had not died prematurely - a measure of premature mortality). Life expectancy and deaths from cancer are not affected by GDP level. When studying infant mortality and potential year lost, in order to avoid the influence of a control variable, it was necessary to group the samples by their GDP per capita level.
Association of Infant Mortality Rates with enrollment rates and education levels
We explored the association of infant mortality rates with the enrollment rates and adult educational levels for all countries (Fig. 2 ). The expectation is that with higher education and employment the infant mortality rate decreases.

Association of Adult Education Levels (ratio) and Enrollment Rates (ratio) with Infant Mortality Rate (per 1000)
Figure 2 depicts the analysis for all countries in the sample. The figure shows the years from 1995 to 2015 on the X axis. It shows two Y-axes with one axis denoting average infant mortality rate (per 1000 live births), and the other showing the rates from 0 to 120 to depict enrollment rates (primary/secondary/tertiary) and education levels (below secondary/upper secondary/tertiary). Regarding the Y axis showing rates over 100, it is worth noting that the enrollment rates denote a ratio of the total enrollment (regardless of age) at a level of education to the official population of the age group in that education level. Therefore, it is possible for the number of children enrolled at a level to exceed the official population of students in the age group for that level (due to repetition or late entry). This can lead to ratios over 100%. The figure shows that in general, all education indicators tend to rise over time, except for adult education level below secondary, which decreases over time. Infant mortality shows a steep decreasing trend over time, which is favorable. In general, countries have increasing health status and education over time, along with decreasing infant mortality rates. This suggests a negative association of education and enrollment rates with mortality rates.
Association of Education Outcomes with life expectancy at birth
We explored if the education outcomes of adult education level (tertiary), school life expectancy (tertiary), and NEET (not in employment, education, or training) rates, affected life expectancy at birth (Fig. 3 ). Our expectation is that adult education and school life expectancy, particularly tertiary, have a positive influence, while NEET has an adverse influence, on life expectancy at birth.

Association of Adult Education Level (Tertiary), NEET rate, School Life Expectancy (Tertiary), with Life Expectancy at Birth
Figure 3 show the relationships between various education indicators (adult education level-tertiary, NEET rate, school life expectancy-tertiary) and life expectancy at birth for all countries in the sample. The figure suggests that life expectancy at birth rises as adult education level (tertiary) and tertiary school life expectancy go up. Life expectancy at birth drops as the NEET rate goes up. In order to extend people’s life expectancy, governments should try to improve tertiary education, and control the number of youths dropping out of school and ending up unemployed (the NEET rate).
Association of Tertiary Enrollment and Education with potential years of life lost
We wanted to explore if the potential years of life lost rates are affected by tertiary enrollment rates and tertiary adult education levels (Fig. 4 ).

Association of Enrollment rate-tertiary (top) and Adult Education Level-Tertiary (bottom) with Potential Years of Life Lost (Y axis)
The two sets of box plots in Fig. 4 compare the enrollment rates with potential years of life lost (above set) and the education level with potential years of life lost (below set). The analysis is for all countries in the sample. As mentioned earlier, the enrollment rates are expressed as ratios and can exceed 100% if the number of children enrolled at a level (regardless of age) exceed the official population of students in the age group for that level. Potential years of life lost represents the average years a person would have lived, had he/she not died prematurely. The results show that with the rise of tertiary adult education level and tertiary enrollment rate, there is a decrease in both value and variation of the potential years of life lost. We can conclude that lower levels in tertiary education adversely affect a country’s health situation in terms of premature mortality.
Association of Tertiary Enrollment and Education with child vaccination rates
We compared the performance of tertiary education level and enrollment rates with the child vaccination rates (Fig. 5 ) to assess if there was a positive impact of education on preventive healthcare.

Association of Adult Education Level-Tertiary and Enrollment Rate-Tertiary with Child Vaccination Rates
In this analysis (Fig. 5 ), we looked for associations of child vaccination rates with tertiary enrollment and tertiary education. The analysis is for all countries in the sample. The color of the bubble represents the tertiary enrollment rate such that the darker the color, the higher the enrollment rate, and the size of the bubble represents the level of tertiary education. The labels inside the bubbles denote the child vaccination rates. The figure shows a general positive association of high child vaccination rate with tertiary enrollment and tertiary education levels. This indicates that countries that have high child vaccination rates tend to be better at tertiary enrollment and have more adults educated in tertiary institutions. Therefore, countries that focus more on tertiary education and enrollment may confer more health awareness in the population, which can be reflected in improved child vaccination rates.
Association of NEET rates (15–19; 20–24) with infant mortality rates and deaths from Cancer
In the realm of child health, we also looked at the infant mortality rates. We explored if infant mortality rates are associated with the NEET rates in different age groups (Fig. 6 ).

Association of Infant Mortality rates with NEET Rates (15–19) and NEET Rates (20–24)
Figure 6 is a scatterplot that explores the correlation between infant mortality and NEET rates in the age groups 15–19 and 20–24. The data is for all countries in the sample. Most data points are clustered in the lower infant mortality and lower NEET rate range. Infant mortality and NEET rates move in the same direction—as infant mortality increases/decrease, the NEET rate goes up/down. The NEET rate for the age group 20–24 has a slightly higher infant mortality rate than the NEET rate for the age group 15–19. This implies that when people in the age group 20–24 are uneducated or unemployed, the implications on infant mortality are higher than in other age groups. This is a reasonable association, since there is the potential to have more people with children in this age group than in the teenage group. To reduce the risk of infant mortality, governments should decrease NEET rates through promotional programs that disseminate the benefits of being educated, employed, and trained [ 7 ]. Additionally, they can offer financial aid to public schools and companies to offer more resources to raise general health awareness in people.
We looked to see if the distribution of population without employment, education, or training (NEET) in various categories of high, medium, and low impacted the rate of deaths from cancer (Fig. 7 ). Our expectation is that high rates of NEET will positively influence deaths from cancer.

Association of Deaths from Cancer and different NEET Rates
The three pie charts in Fig. 7 show the distribution of deaths from cancer in groups of countries with different NEET rates (high, medium, and low). The analysis includes all countries in the sample. The expectation was that high rates of NEET would be associated with high rates of cancer deaths. Our results, however, show that countries with medium NEET rates tend to have the highest deaths from cancer. Countries with high NEET rates have the lowest deaths from cancer among the three groups. Contrary to expectations, countries with low NEET rates do not show the lowest death rates from cancer. A possible explanation for this can be attributed to the fact that in this group, the people in the labor force may be suffering from work-related hazards including stress, that endanger their health.
Association between adult education levels and health expenditure
It is interesting to note the relationship between health expenditure and adult education levels (Fig. 8 ). We expect them to be positively associated.

Association of Health Expenditure and Adult Education Level-Tertiary & Upper Secondary
Figure 8 shows a heat map with the number of countries in different combinations of groups between tertiary and upper-secondary adult education level. We emphasize the higher levels of adult education. The color of the square shows the average of health expenditure. The plot shows that most of the countries are divided into two clusters. One cluster has a high tertiary education level as well as a high upper-secondary education level and it has high average health expenditure. The other cluster has relatively low tertiary and upper secondary education level with low average health expenditure. Overall, the figure shows a positive correlation between adult education level and compulsory health expenditure. Governments of countries with low levels of education should allocate more health expenditure, which will have an influence on the educational levels. Alternatively, to improve public health, governments can frame educational policies to improve the overall national education level, which then produces more health awareness, contributing to national healthcare.
Association of Compulsory Health Expenditure with NEET rates by country and region
Having explored the relationship between health expenditure and adult education, we then explored the relationship between health expenditure and NEET rates of different countries (Fig. 9 ). We expect compulsory health expenditure to be negatively associated with NEET rates.

Association between Compulsory Health Expenditure and NEET Rate by Country and Region
In Fig. 9 , each box represents a country or region; the size of the box indicates the extent of compulsory health expenditure such that a larger box implies that the country has greater compulsory health expenditure. The intensity of the color of the box represents the NEET rate such that the darker color implies a higher NEET rate. Turkey has the highest NEET rate with low health expenditure. Most European countries such as France, Belgium, Sweden, and Norway have low NEET rates and high health expenditure. The chart shows a general association between low compulsory health expenditure and high NEET rates. The relationship, however, is not consistent, as there are countries with high NEET and high health expenditures. Our suggestion is for most countries to improve the social education for the youth through free training programs and other means to effectively improve the public health while they attempt to raise the compulsory expenditure.
Distribution of life expectancy at birth and tertiary enrollment rate
The distribution of enrollment rate (tertiary) and life expectancy of all the countries in the sample can give an idea of the current status of both education and health (Fig. 10 ). We expect these to be positively associated.

Distribution of Life Expectancy at Birth (years) and Tertiary Enrollment Rate
Figure 10 shows two histograms with the lines representing the distribution of life expectancy at birth and the tertiary enrollment rate of all the countries. The distribution of life expectancy at birth is skewed right, which means most of the countries have quite a high life expectancy and there are few countries with a very low life expectancy. The tertiary enrollment rate has a good distribution, which is closer to a normal distribution. Governments of countries with an extremely low life expectancy should try to identify the cause of this problem and take actions in time to improve the overall national health.
Comparison of adult education levels and deaths from Cancer at various levels of GDP per capita
We wanted to see if various levels of GDP per capita influence the levels of adult education and deaths from cancer in countries (Fig. 11 ).

Comparison of Adult Education Levels and Deaths from Cancer at various levels of GDP per capita
Figure 11 shows the distribution of various adult education levels for countries by groups of GDP per capita. The plot shows that as GDP grows, the level of below-secondary adult education becomes lower, and the level of tertiary education gets higher. The upper-secondary education level is constant among all the groups. The implication is that tertiary education is the most important factor among all the education levels for a country to improve its economic power and health level. Countries should therefore focus on tertiary education as a driver of economic development. As for deaths from cancer, countries with lower GDP have higher death rates, indicating the negative association between economic development and deaths from cancer.
Distribution of infant mortality rates by continent
Infant mortality is an important indicator of a country’s health status. Figure 12 shows the distribution of infant mortality for the continents of Asia, Europe, Oceania, North and South America. We grouped the countries in each continent into high, medium, and low, based on infant mortality rates.

Distribution of Infant Mortality rates by Continent
In Fig. 12 , each bar represents a continent. All countries fall into three groups (high, medium, and low) based on infant mortality rates. South America has the highest infant mortality, followed by Asia, Europe, and Oceania. North America falls in the medium range of infant mortality. South American countries, in general, should strive to improve infant mortality. While Europe, in general, has the lowest infant mortality rates, there are some countries that have high rates as depicted.
Association between child vaccination rates and NEET rates
We looked at the association between child vaccination rates and NEET rates in various countries (Fig. 13 ). We expect countries that have high NEET rates to have low child vaccination rates.

Association between Child Vaccination Rates and NEET rates
Figure 13 displays the child vaccination rates in the first map and the NEET rates in the second map, for all countries. The darker green color shows countries with higher rates of vaccination and the darker red represents those with higher NEET rates. It can be seen that in general, the countries with lower NEET also have better vaccination rates. Examples are USA, UK, Iceland, France, and North European countries. Countries should therefore strive to reduce NEET rates by enrolling a good proportion of the youth into initiatives or programs that will help them be more productive in the future, and be able to afford preventive healthcare for the families, particularly, the children.
Average smoking rate in different continents over time
We compared the trend of average smoking rate for the years 1995–201 for the continents in the sample (Fig. 14 ).

Trend of average smoking rate in different continents from 1995 to 2015
Figure 14 depicts the line charts of average smoking rates for the continents of Asia, Europe, Oceania, North and South America. All the lines show an overall downward trend, which indicates that the average smoking rate decreases with time. The trend illustrates that people have become more health conscious and realize the harmful effects of smoking over time. However, the smoking rate in Europe (EU) is consistently higher than that in other continents, while the smoking rate in North America (NA) is consistently lower over the years. Governments in Europe should pay attention to the usage of tobacco and increase health consciousness among the public.
Association between adult education levels and deaths from Cancer
We explored if adult education levels (below-secondary, upper-secondary, and tertiary) are associated with deaths from cancer (Fig. 15 ) such that higher levels of education will mitigate the rates of deaths from cancer, due to increased awareness and proactive health behavior.

Association of deaths from cancer with adult education levels
Figure 15 shows the correlations of deaths from cancer among the three adult education levels, for all countries in the sample. It is obvious that below-secondary and tertiary adult education levels have a negative correlation with deaths from cancer, while the upper-secondary adult education level shows a positive correlation. Barring upper-secondary results, we can surmise that in general, as education level goes higher, the deaths from cancer will decrease. The rationale for this could be that education fosters more health awareness and encourages people to adopt healthy behavioral practices. Governments should therefore pay attention to frame policies that promote education. However, the counterintuitive result of the positive correlation between upper-secondary levels of adult education with the deaths from cancer warrants more investigation.
We drilled down further into the correlation between the upper-secondary education level and deaths from cancer. Figure 16 shows this correlation, along with a breakdown of the total number of records for each continent, to see if there is an explanation for the unique result.

Association between deaths from cancer and adult education level-upper secondary
Figure 16 shows a dashboard containing two graphs - a scatterplot of the correlation between deaths from cancer and education level, and a bar graph showing the breakdown of the total sample by continent. We included a breakdown by continent in order to explore variances that may clarify or explain the positive association for deaths from cancer with the upper-secondary education level. The scatterplot shows that for the European Union (EU) the points are much more scattered than for the other continents. Also, the correlation between deaths and education level for the EU is positive. The bottom bar graph depicts how the sample contains a disproportionately high number of records for the EU than for other continents. It is possible that this may have influenced the results of the correlation. The governments in the EU should investigate the reasons behind this phenomenon. Also, we defer to future research to explore this in greater detail by incorporating other socioeconomic parameters that may have to be factored into the relationship.
Association between average tertiary school life expectancy and health expenditure
We moved our focus to the trends of tertiary school life expectancy and health expenditure from 1995 to 2015 (Fig. 17 ) to check for positive associations.

Association between Average Tertiary School Life Expectancy and Health Expenditure
Figure 17 is a combination chart explaining the trends of tertiary school life expectancy and health expenditure, for all countries in the sample. The rationale is that if there is a positive association between the two, it would be worthwhile for the government to allocate more resources towards health expenditure. Both tertiary school life expectancy and health expenditure show an increase over the years from 1995 to 2015. Our additional analysis shows that they continue to increase even after 2015. Hence, governments are encouraged to increase the health expenditure in order to see gains in tertiary school life expectancy, which will have positive implications for national health. Given that the measured effects of education are large, investments in education might prove to be a cost-effective means of achieving better health.
Our results reveal how interlinked education and health can be. We show how a country can improve its health scenario by focusing on appropriate indicators of education. Countries with higher education levels are more likely to have better national health conditions. Among the adult education levels, tertiary education is the most critical indicator influencing healthcare in terms of infant mortality, life expectancy, child vaccination rates, and enrollment rates. Our results emphasize the role that education plays in the potential years of life lost, which is a measure that represents the average years a person would have lived had he/she not died prematurely. In addition to mortality rate, an economy needs to consider this indicator as a measure of health quality.
Other educational indicators that are major drivers of health include school life expectancy, particularly at the tertiary level. In order to improve the school life expectancy of the population, governments should control the number of youths ending up unemployed, dropping out of school, and without skills or training (the NEET rate). Education allows people to gain skills/abilities and knowledge on general health, enhancing their awareness of healthy behaviors and preventive care. By targeting promotions and campaigns that emphasize the importance of skills and employment, governments can reduce the NEET rates. And, by reducing the NEET rates, governments have the potential to address a broad array of vulnerabilities among youth, ranging from unemployment, early school dropouts, and labor market discouragement, which are all social issues that warrant attention in a growing economy.
We also bring to light the health disparities across countries and suggest implications for governments to target educational interventions that can reduce inequalities and improve health, at a macro level. The health effects of education are at the grass roots level - creating better overall self-awareness on personal health and making healthcare more accessible.
Scope and limitations
Our research suffers from a few limitations. For one, the number of countries is limited, and being that the data are primarily drawn from OECD, they pertain to the continent of Europe. We also considered a limited set of variables. A more extensive study can encompass a larger range of variables drawn from heterogeneous sources. With the objective of acquiring a macro perspective on the education–health association, we incorporated some dependent variables that may not traditionally be viewed as pure health parameters. For example, the variable potential years of life lost is affected by premature deaths that may be caused by non-health related factors too. Also there may be some intervening variables in the education–health relationship that need to be considered. Lastly, while our study explores associations and relationships between variables, it does not investigate causality.
Conclusions and future research
Both education and health are at the center of individual and population health and well-being. Conceptualizations of both phenomena should go beyond the individual focus to incorporate and consider the social context and structure within which the education–health relationship is embedded. Such an approach calls for a combination of interdisciplinary research, novel conceptual models, and rich data sources. As health differences are widening across the world, there is need for new directions in research and policy on health returns on education and vice versa. In developing interventions and policies, governments would do well to keep in mind the dual role played by education—as a driver of opportunity as well as a reproducer of inequality [ 36 ]. Reducing these macro-level inequalities requires interventions directed at a macro level. Researchers and policy makers have mutual responsibilities in this endeavor, with researchers investigating and communicating the insights and recommendations to policy makers, and policy makers conveying the challenges and needs of health and educational practices to researchers. Researchers can leverage national differences in the political system to study the impact of various welfare systems on the education–health association. In terms of investment in education, we make a call for governments to focus on education in the early stages of life course so as to prevent the reproduction of social inequalities and change upcoming educational trajectories; we also urge governments to make efforts to mitigate the rising dropout rate in postsecondary enrollment that often leads to detrimental health (e.g., due to stress or rising student debt). There is a need to look into the circumstances that can modify the postsecondary experience of youth so as to improve their health.
Our study offers several prospects for future research. Future research can incorporate geographic and environmental variables—such as the quality of air level or latitude—for additional analysis. Also, we can incorporate data from other sources to include more countries and more variables, especially non-European ones, so as to increase the breadth of analysis. In terms of methodology, future studies can deploy meta-regression analysis to compare the relationships between health and some macro-level socioeconomic indicators [ 13 ]. Future research should also expand beyond the individual to the social context in which education and health are situated. Such an approach will help generate findings that will inform effective educational and health policies and interventions to reduce disparities.
Availability of data and materials
The dataset analyzed during the current study is available from the corresponding author on reasonable request.
Abbreviations
Fundamental Cause Theory
Human Capital Theory
Not in Employment, Education, or Training
Organization for Economic Cooperation and Development
Socio-economic status
Andersen RM, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Mem Fund Q Health Soc. 1973;51(1):95–124.
Article CAS Google Scholar
Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Social Behav. 1995;36(1):1–10.
Baker DP. The Schooled Society: The Educational Transformation of Global Culture. Stanford, CA: Stanford Univ. Press: 2014; 360.
Becker GS. Human capital: a theoretical and empirical analysis, with special reference to education. Chicago: Univ. Chicago Press; 1964.
Google Scholar
Berkman LF, Syme SL. Social networks, host resistance, and mortality: a nine-year follow-up study of Alameda County residents. Oxford Acad J. 1979;109(2):186–204.
CAS Google Scholar
Crimmins EM, Kim JK, Vasunilashorn S. Biodemography: new approaches to understanding trends and differences in population health and mortality. Demography. 2010;47:S41–64.
Article Google Scholar
Spence M. Job market signalling. The Quarterly J Econ. 1973;87:355–79.
Cutler DM, Lleras-Muney A. Education and Health: Evaluating Theories and Evidence: NBER Working Papers; 2006. p. 12352.
Feinstein L. What are the effects of education on health? OECD Proceedings of the Copenhagen Symposium; 2006 . .
Folkman S, Lazarus RS. An analysis of coping in a middle-aged community sample. J Health Soc Behav. 1980;21(3):219–39.
Freedman VA, Martin LG. The role of education in explaining and forecasting trends in functional limitations among older Americans. Demography. 1999;36(4):461–73.
Freese J, Lutfey K. Fundamental causality: challenges of an animating concept for medical sociology. In: Pescosolido BA, Martin JK, McLeod JD, Rogers A, editors. Handbook of the Sociology of Health, Illness, and Healing: a blueprint for the 21st century. New York: Springer; 2011. p. 67–81.
Chapter Google Scholar
Fouweather T, Gillies C, Wohland P, Van Oyen H, Nusselde W, Robine J, Cambois E, Jagger C. Comparison of socio-economic indicators explaining inequalities in healthy life years at age 50 in Europe: 2005 and 2010. Eur J Pub Health. 2015;25:978–83.
George LK, Gwyther LP. Caregiver Weil-being: a multidimensional examination of family caregivers of demented adults. Gerontologist. 1986;26(3):253–9.
Goldman D, Smith JP. The increasing value of education to health. Soc Sc Med. 2011;72(10):1728–37.
Harper AC, Lambert LJ. The health of populations: an introduction. New York: Springer Publishing Company; 1994.
Health 2020: Education and health through the life-course. WHO Europe Sector Brief on Education Health; 2015. http://www.euro.who.int/__data/assets/pdf_file/0007/324619/Health-2020-Education-and-health-through-the-life-course-en.pdf?ua=1 .
Kino S, Bernabé E, Sabbah W. The role of healthcare and education systems in co-occurrence of health risk behaviours in 27 European countries. Eur J Public Health. 2018;28(1):186–92.
Landerman LR, Burns BJ, Swartz MS, Wagner HR, George LK. The relationship between insurance coverage and psychiatric disorder in predicting use of mental health services. Am J Psychol. 1994;151(12):1785.
Lynch SM. Cohort and life-course patterns in the relationship between education and health: a hierarchical approach. Demography. 2003;40(2):309–31.
Mackenbach J, Kunst A. Measuring the magnitude of socio-economic inequalities in health: an overview of available measures illustrated with two examples from Europe. Soc Sci Med. 1997;44(6):757–71. https://doi.org/10.1016/S0277-9536(96)00073-1 .
Article CAS PubMed Google Scholar
Manton KG, Corder L, Stallard E. Chronic disability trends in elderly United States populations: 1982-1994. Natl Acad Sci. 1997;94(6):2593–8.
Mirowski J, Ross CE. Education, learned effectiveness and health. London Rev Edu. 2005;3(3):205–20.
Montez JK, Berkman LF. Trends in the educational gradient of mortality among US adults aged 45 to 84 years: bringing regional context into the explanation. Am J Pub Health. 2014;104(1):e82–90.
Montez JK, Zajacova A. Trends in mortality risk by education level and cause of death among US white women from 1986 to 2006. Am J Pub Health. 2013;103:473–9.
Olshansky SJ, Antonucci T, Berkman L, Binstock RH, Boersch-Supan A, Cacioppo JT, Carnes BA, Carstensen LL, Fried LP, Goldman DP, Jackson J, Kohli M, Rother J, Zheng Y, Rowe J. Differences in life expectancy due to race and educational differences are widening, and many may not catch up. Health Aff. 2012;31(8):1803–13.
Pamuk ER. Social-class inequality in infant mortality in England and Wales from 1921 to 1980. Eur J Popul 1988; 4 , 1–21, https://doi.org/10.1007/BF01797104.
Phelan JC , Link BG , Tehranifar P . Social conditions as fundamental causes of health inequalities: Theory, evidence, and policy implications . J Health Soc Behav 2010 ; 51 : S28 S40 . doi : 10.1177/0022146510383498.
Renard F, Devleesschauwer B, Speybroeck N, Deboosere P. Monitoring health inequalities when the socio-economic composition changes: are the slope and relative indices of inequality appropriate? Results of a simulation study. BMC Public Health 2019; 19: 662. https://doi.org/10.1186/s12889-019-6980-1.
Ro A, Geronimus A, Bound J, Griffith D, Gee G. Educational gradients in five Asian immigrant populations: do country of origin, duration and generational status moderate the education-health relationship? Prev Med Rep. 2016;4:338–43.
Ross CE, Wu CL. The links between education and health. Am Soc Rev. 1995;60(5):719–45.
Shiels MS, Chernyavskiy P, Anderson WF, Best AF, Haozous EA. Diverging trends in premature mortality in the U.S. by sex, race, and ethnicity in the 21st century. Lancet. 2017;389:1043–54.
Tsou MT. Association of Education, health behaviors, concerns, and knowledge with metabolic syndrome among urban elderly in one medical Center in Taiwan. Int J Gerontology. 2017;11(3:138–43.
Wheaton B. Stress, personal coping resources, and psychiatric symptoms: an investigation of interactive models. J Health Soc Behav. 1983;24(3):208–29.
Williams DR, Collins C. US socioeconomic and racial differences in health: patterns and explanations. Ann Rev Soc. 1995;21:349–86.
Zajacova A, Lawrence EM. The relationship between education and health: reducing disparities through a contextual approach. Ann Rev Pub Health. 2018;39:273–89.
Zimmerman EB, Woolf SH. Understanding the relationship between education and health. Discussion Paper, Inst Med. Washington DC; 2014. https://nam.edu/wp-content/uploads/2015/06/BPH-UnderstandingTheRelationship1.pdf .
Zhong H. An over time analysis on the mechanisms behind the education–health gradients in China. China Econ Rev. 2015;34(C):135–49.
Download references
Acknowledgements
Not applicable.
Author information
Authors and affiliations.
Koppelman School of Business, Brooklyn College of the City University of New York, 2900 Bedford Ave, Brooklyn, NY, 11210, USA
Viju Raghupathi
Gabelli School of Business, Fordham University, 140 W. 62nd Street, New York, NY, 10023, USA
Wullianallur Raghupathi
You can also search for this author in PubMed Google Scholar
Contributions
Both authors contributed equally to all parts of the manuscript.
Corresponding author
Correspondence to Viju Raghupathi .
Ethics declarations
Ethics approval and consent to participate, consent for publication, competing interests.
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Raghupathi, V., Raghupathi, W. The influence of education on health: an empirical assessment of OECD countries for the period 1995–2015. Arch Public Health 78 , 20 (2020). https://doi.org/10.1186/s13690-020-00402-5
Download citation
Received : 16 October 2019
Accepted : 26 February 2020
Published : 06 April 2020
DOI : https://doi.org/10.1186/s13690-020-00402-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Education level
- Enrollment rate
- Life expectancy
- Potential years of life lost
- Infant mortality
- Deaths from cancer
Archives of Public Health
ISSN: 2049-3258
- General enquiries: [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
The PMC website is updating on October 15, 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- NAM Perspect
- v.2020; 2020
Health Literacy and Health Education in Schools: Collaboration for Action
M. elaine auld.
Society for Public Health Education
Marin P. Allen
National Institutes of Health (ret.)
Cicily Hampton
University of North Carolina at Charlotte
J. Henry Montes
American Public Health Association
Cherylee Sherry
Minnesota Department of Health
Angela D. Mickalide
American College of Preventive Medicine
Robert A. Logan
U.S. National Library of Medicine and University of Missouri-Columbia
Wilma Alvarado-Little
New York State Department of Health
July 20, 2020
Introduction
This NAM Perspectives paper provides an overview of health education in schools and challenges encountered in enacting evidence-based health education; timely policy-related opportunities for strengthening school health education curricula, including incorporation of essential health literacy concepts and skills; and case studies demonstrating the successful integration of school health education and health literacy in chronic disease management. The authors of this manuscript conclude with a call to action to identify upstream, systems-level changes that will strengthen the integration of both health literacy and school health education to improve the health of future generations. The COVID-19 epidemic [ 10 ] dramatically demonstrates the need for children, as well as adults, to develop new and specific health knowledge and behaviors and calls for increased integration of health education with schools and communities.
Enhancing the education and health of school-age children is a critical issue for the continued well-being of our nation. The 2004 Institute of Medicine (IOM, now the National Academies of Sciences, Engineering, and Medicine [NASEM]) report, Health Literacy: A Prescription to End Confusion [ 27 ] noted the education system as one major pathway for improving health literacy by integrating health knowledge and skills into the existing curricula of kindergarten through 12th grade classes. The NASEM Roundtable on Health Literacy has held multiple workshops and forums to “inform, inspire, and activate a wide variety of stakeholders to support the development, implementation, and sharing of evidence-based health literacy practices and policies” [ 37 ]. This paper strives to present current evidence and examples of how the collaboration between health education and health literacy disciplines can strengthen K–12 education, promote improved health, and foster dialogue among school officials, public health officials, teachers, parents, students, and other stakeholders.
This discussion also expands on a previous NAM Perspectives paper, which identified commonalities and differences in the fields of health education, health literacy, and health communication and called for collaboration across the disciplines to “engage learners in both formal and informal health educational settings across the life span” [ 1 ]. To improve overall health literacy, i.e., “the capacity of individuals to obtain, process, and understand basic health information and services needed to make appropriate health decisions” [ 42 ], it is important to start with youth, when life-long health habits are first being formed.
Another recent NAM Perspectives paper proposed the expansion of the definition of health literacy to include broader contextual factors, including issues that impact K–12 health education efforts like state rather than federal control of education priorities and administration, and subsequent state- or local-level laws that impact specific school policies and practices [ 39 ]. In addition to addressing individual needs and abilities, socio-ecological factors can impact a student’s health. For example, the Centers for Disease Control and Prevention (CDC) uses a four-level social-ecological model to describe “the complex interplay” of (1) individuals (biological and personal history factors), (2) relationships (close peers, family members), (3) community (settings such as neighborhoods, schools, after-school locations), and (4) societal factors (cultural norms, policies related to health and education, or inequalities between groups in societies) that put one at risk or prevent him/her from experiencing negative health outcomes [ 11 ]. Also worth examining are protective factors that help children and adolescents avoid behaviors that place them at risk for adverse health and educational outcomes (e.g., self-efficacy, self-esteem, parental support, adult mentors, and youth programs) [ 21 , 59 ].
Recognizing the influence of this larger social context on learning and health can help catalyze both individual and community-based solutions. For example, students with chronic illnesses such as asthma, which can affect their school attendance, can be educated about the impact of air quality or housing (e.g., mold, mites) in exacerbating their condition. Students in varied locations and at a range of ages continue, often with the guidance of adults, to take health-related social action. Various local, national, and international examples illustrate high schoolers taking social action related to health issues such as tobacco, gun safety, and climate change [ 18 , 21 , 57 ].
By employing a broad approach to K–12 education (i.e., using combined principles of health education and health literacy), the authors of this manuscript foresee a template for the integration of skills and abilities needed by both school health professionals and children and parents to increase health knowledge for a lifetime of improved health [ 1 , 29 , 31 ].
The right measurements to evaluate success and areas that need improvement must be clearly identified because in all matters related to health education and health literacy, it is vital to document the linkages between informed decisions and actions. Often, individuals are presumed to be making informed decisions when actually broader socio-ecological factors are predominant behavioral influences (e.g., an individual who is overweight but has never learned about food label-ling and lives in a community where there are no safe places to be physically active).
Health Education in Schools
Standardized and broadly adopted strategies for how health education is implemented in schools—and by whom and on what schedule—is a continuing challenge. Although the principles of health literacy are inherently important to any instruction in schools and in community settings, the most effective way to incorporate those principles in existing and differing systems becomes a key to successful health education for children and young people.
The concept of incorporating health education into the formal education system dates to the Renaissance. However, it did not emerge in the United States until several centuries later [ 26 ]. In the early 19th century, Horace Mann advocated for school-based health instruction, while William Alcott also underscored the contributions of health services and the school environment to children’s health and well-being [ 17 ]. Public health pioneer Lemuel Shattuck wrote in 1850 that “every child should be taught early in life, that to preserve his own life and his own health and the lives of others, is one of the most important and abiding duties” [ 43 ]. During this same time, Harvard University and other higher education institutions with teacher preparation programs began including hygiene (health) education in their curricula.
Despite such early historical recognition, in the mid-1960s, the School Health Education Study documented serious disarray in the organization and administration of school health education programs [ 45 ]. A renewed call to action, several decades later, introduced the concepts of comprehensive school health programs and school health education [ 26 ].
From 1998 through 2014, the CDC and other organizations began using the term “coordinated school health programs” to encompass eight components affecting children’s health in schools, including nutrition, health services, and health instruction. Unfortunately, the term was not broadly embraced by the educational sector, and in 2014, CDC and ASCD (formerly the Association for Supervision and Curriculum Development) unveiled the Whole School, Whole Community, Whole Child (WSCC) framework [ 36 ]. This framework has ten components, including health education, which aims to ensure that each student is healthy, safe, engaged, supported, and challenged. Among the foundational tenets of the framework is ensuring that every student enters school healthy and, while there, learns about and practices a healthy lifestyle.
At its core, health education is defined as “any combination of planned learning experiences using evidence based practices and/or sound theories that provide the opportunity to acquire knowledge, attitudes, and skills needed to adopt and maintain healthy behaviors” [ 3 ]. Included are a variety of physical, social, emotional, and other components focused on reducing health-risk behaviors and promoting healthy decision making. Health education curricula emphasize a skills-based approach to help students practice and advocate for their health needs, as well as the needs of their families and their communities. These skills help children and adolescents find and evaluate health information needed for making informed health decisions and ultimately provide the foundation of how to advocate for their own well-being throughout their lives.
In the last 40 years, many studies have documented the relationship between student health and academic outcomes [ 29 , 40 , 41 ]. Health-related problems can diminish a student’s motivation and ability to learn [ 4 ]. Complications with vision, hearing, asthma, occurrences of teen pregnancy, aggression and violence, lack of physical activity, and low cognitive and emotional ability can reduce academic success [ 4 ].
To date, there have been no long-term sequential studies of the impact of K–12 health education curricula on health literacy or health outcomes. However, research shows that students who participate in health education curricula in combination with other interventions as part of the coordinated school health model (i.e., physical activity, improved nutrition, and/or family engagement) have reduced rates of obesity and/or improved health-promoting behaviors [ 25 , 30 , 34 ]. In addition, school health education has been shown to prevent tobacco and alcohol use and prevent dating aggression and violence. Teaching social and emotional skills improves academic behaviors of students, increases motivation to do well in school, enhances performance on achievement tests and grades, and improves high school graduation rates.
As with other content areas, it is up to the state and/or local government to determine what should be taught, under the 10th Amendment to the US Constitution [ 48 ]. However, both public and private organizations have produced seminal documents to help guide states and local governments in selecting health education curricula. First published in 1995 and updated in 2004, the National Health Education Standards (NHES) framework comprises eight health education foundations for what students in kindergarten through 12th grade should know and be able to do to promote personal, family, and community health (see Table 1 ) [ 12 ]. The NHES framework serves as a reference for school administrators, teachers, and others addressing health literacy in developing or selecting curricula, allotting instructional resources, and assessing student achievement and progress. The NHES framework contains written expectations for what students should know and be able to do by grades 2, 5, 8, and 12 to promote personal, family, and community health.
| Standard 1 | Students will comprehend concepts related to health promotion and disease prevention to enhance health. |
| Standard 2 | Students will analyze the influence of family, peers, culture, media, technology, and other factors on health behaviors. |
| Standard 3 | Students will demonstrate the ability to access valid information, products, and services to enhance health. |
| Standard 4 | Students will demonstrate the ability to use interpersonal communication skills to enhance health and avoid or reduce health risks. |
| Standard 5 | Students will demonstrate the ability to use decision-making skills to enhance health. |
| Standard 6 | Students will demonstrate the ability to use goal-setting skills to enhance health. |
| Standard 7 | Students will demonstrate the ability to practice health-enhancing behaviors and avoid or reduce health risks. |
| Standard 8 | Students will demonstrate the ability to advocate for personal, family, and community health. |
SOURCE: Centers for Disease Control and Prevention. 2020. National Health Education Standards. Available at: National Health Education Standards Website. https://www.cdc.gov/healthyschools/sher/standards/index.htm (accessed June 19, 2020).
The Coordinated Approach to Child Health (CATCH) model, which was first developed in the late 1980s with funds by the National Heart, Lung, and Blood Institute, serves to implement the NHES framework and was the largest school-based health promotion study ever conducted in the United States. CATCH has 25 years of continuous research and development of its programs [ 24 ] and aligns with the WSCC framework. Individualized programs like the CATCH model develop programming based on the NHES framework at the local level, so that local control still exists, but the mix and depth of topics can vary based on need and composition of the community.
Based on reviews of effective programs and curricula and experts in the field of health education, CDC recommends that today’s state-of-the-art health education curricula emphasize four core elements: “Teaching functional health information (essential knowledge); shaping personal values and beliefs that support healthy behaviors; shaping group norms that value a healthy lifestyle; and developing the essential health skills necessary to adopt, practice, and maintain health enhancing behavior” [ 13 ]. In addition to the 15 characteristics presented in Box 1 , the CDC website has more detailed explanations and examples of how the statements could be put into practice in the classroom. For example, a curriculum that “builds personal competence, social competence, and self-efficacy by addressing skills” would be expected to guide students through a series of developmental steps that discuss the importance of the skill, its relevance, and relationship to other learned skills; present steps for developing the skill; model the skill; practice and rehearse the skill using real-life scenarios; and provide feedback and reinforcement.
Characteristics of an Effective Health Education Curriculum
- 1. Focuses on clear health goals and related behavioral outcomes.
- 2. Is research-based and theory-driven.
- 3. Addresses individual values, attitudes, and beliefs.
- 4. Addresses individual and group norms that support health-enhancing behaviors.
- 5. Focuses on reinforcing protective factors and increasing perceptions of personal risk and harmfulness of engaging in specific unhealthy practices and behaviors.
- 6. Addresses social pressures and influences.
- 7. Builds personal competence, social competence, and self-efficacy by addressing skills.
- 8. Provides functional health knowledge that is basic, accurate, and directly contributes to health-promoting decisions and behaviors.
- 9. Uses strategies designed to personalize information and engage students.
- 10. Provides age-appropriate and developmentally appropriate information, learning strategies, teaching methods, and materials.
- 11. Incorporates learning strategies, teaching methods, and materials that are culturally inclusive.
- 12. Provides adequate time for instruction and learning.
- 13. Provides opportunities to reinforce skills and positive health behaviors.
- 14. Provides opportunities to make positive connections with influential others.
- 15. Includes teacher information and plans for professional development and training that enhance effectiveness of instruction and student learning.
SOURCE: Centers for Disease Control and Prevention. 2020. Characteristics of an Effective Health Education Curriculum. Available at: https://www.cdc.gov/healthyschools/sher/characteristics/index.htm (accessed June 19, 2020.)
In addition, CDC has developed a Health Education Curriculum Analysis Tool [ 14 ] to help schools conduct an analysis of health education curricula based on the NHES framework and the Characteristics of an Effective Health Education Curriculum.
Despite CDC’s extensive efforts during the past 40 years to help schools implement effective school health education and other components of the broader school health program, the integration of health education into schools has continued to fall short in most US states and cities. According to the CDC’s 2016 School Health Profiles report, the percentage of schools that required any health education instruction for students in any of grades 6 through 12 declined. For example, 8 in 10 US school districts only required teaching about violence prevention in elementary schools and violence prevention plus tobacco use prevention in middle schools, while instruction in only seven health topics was required in most high schools [ 6 ].
Although 8 of every 10 districts required schools to follow either national, state, or district health education standards, just over a third assessed attainment of health standards at the elementary level while only half did so at the middle and high school levels [ 6 ]. No Child Left Behind legislation, enacted in 2002, emphasized testing of core subjects, such as reading, science, and math, which resulted in marginalization of other subjects, including health education [ 22 , 31 ]. Academic subjects that are not considered “core” are at risk of being eliminated as public school principals and administrators struggle to meet adequate yearly progress for core subjects, now required to maintain federal funding.
In addition to the quality and quantity of health education taught in schools, there are numerous problems related to those considered qualified to provide instruction [ 5 , 7 ]. Many school and university administrators lack an understanding of the distinction between health education and physical education (PE) [ 9 , 16 , 19 ] and consider PE teachers to be qualified to teach health education. Yet the two disciplines differ regarding national standards, student learning outcomes, instructional content and methods, and student assessment [ 5 ]. Kolbe notes that making gains in school health education will require more interdisciplinary collaboration in higher education (e.g., those training the public health workforce, the education workforce, school nurses, pediatricians) [ 29 ]. Yet faculty who train various school health professionals usually work within one university college, focus on one school health component, and affiliate with one national professional organization. In addition, Kolbe notes that health education teachers in today’s workforce often lack support and resources for in-service professional development.
Promising Opportunities for Strengthening School Health Education
Comprehensive health education can increase health literacy, which has been estimated to cost the nation $1.6 to $3.6 trillion dollars annually [ 54 ]. The National Action Plan to Improve Health Literacy by the US Department of Health and Human Services (HHS) includes the goal to “Incorporate accurate, standards-based, and developmentally appropriate health and science information and curricula in childcare and education through the university level” [ 49 ].
HHS’s Healthy People Framework presents another significant opportunity for tracking health in education as well as health literacy. The Healthy People initiative launched officially in 1979 with the publication of Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention [ 50 ]. This national effort establishes 10-year goals and objectives to improve the health and well-being of people in the United States. Since its inception, Healthy People has undertaken extensive efforts to collect data, assess progress, and engage multi-stakeholder feedback to set objectives for the next ten years. The Healthy People 2020 objectives were self-described as having “input from public health and prevention experts, a wide range of federal, state, and local government officials, a consortium of more than 2,000 organizations, and perhaps most importantly, the public” [ 51 ]. In addition to other childhood and adolescent objectives (e.g., nutrition, physical activity, vaccinations), Healthy People 2020 specified social determinants as a major topic for the first time. A leading health indicator for social determinants was “students graduating from high school within 4 years of starting 9th grade (AH-5.1)” [ 52 ]. The Secretary’s Advisory Committee report on the Healthy People 2030 objectives includes the goal to “eliminate health disparities, achieve health equity, and attain health literacy to improve the health and well-being of all” [ 53 ]. The national objectives are expected to be released in summer 2020 and will help catalyze “leadership, key constituents, and the public across multiple sectors to take action and design policies that improve the health and well-being of all” [ 53 ].
In terms of supports in federal legislation, the Every Student Succeeds Act (ESSA) of 2015 recognized health education as a distinct discipline for the first time and designated it as a “well-rounded” education subject [ 2 , 22 ]. According to Department of Education guidelines, each state must submit a plan that includes four academic indicators that include proficiency in math, English, and English-language proficiency. High schools also must use their graduation rates as their fourth indicator, while elementary and middle schools may use another academic indicator. In addition, states must specify at least one nonacademic indicator to measure school quality or school success, such as health education. Under the law, federal funding also is available for in-service instruction for teachers in well-rounded education subjects such as health education. These two items open additional pathways for both identifying existing or added programs and having the capacity to collect data.
While several states have chosen access to physical education, physical fitness, or school climate as their nonacademic indicators of school success, the majority (36 states and the District of Columbia) have elected to use chronic absenteeism [ 2 ]. Given the underlying causal connection between student health and chronic absenteeism, absenteeism as an indicator represents a significant opportunity to raise awareness of chronic health conditions or other issues (e.g., student social/emotional concerns around bullying, school safety) that contribute to absenteeism. It also represents a significant opportunity for schools to work with stakeholders to prevent and manage such health conditions through school health education and other WSCC strategies to improve school health. Educators are more likely to support comprehensive health education if they are made aware of its immediate benefits related to student learning (e.g., less disruptive behavior, improved attention) and maintaining safe social and emotional school climates [ 31 ].
In an assessment of how states are addressing WSCC, Child Trends reported that health education is either encouraged or required for all grades in all states’ laws, with nutrition (40 states) and personal health (44 states) as the most prominent topics [ 15 ]. However, the depth and breadth of such instruction in schools is not known, nor if health education is being taught by qualified teachers. In 25 states, laws address or otherwise incorporate the NHES as part of the state health education curriculum.
The authors’ review of state 2017–2018 ESSA plans, analyzed by the organization Cairn, showed nine states that have specifically identified health education as one of its required well-rounded subjects (Florida, Georgia, Indiana, Louisiana, Maine, Maryland, Nevada, North Dakota, and Tennessee) [ 8 ]. Cairn recommends that most states include health education and physical education in state accountability systems, school report card indicators, school improvement plans, professional development plans, needs assessment tools, and/or prioritized funding under Title IV, Part A.
In 2019, representatives of the National Committee on the Future of School Health Education, sponsored by the Society for Public Health Education (SOPHE) and the American School Health Association (ASHA), published a dozen recommendations for strengthening school health education [ 5 , 31 , 55 ]. The recommendations addressed issues such as developing and adopting standardized measures of health literacy in children and including them in state accountability systems; changing policies, practices, and systems for quality school health education (e.g., establishing Director of School Health Education positions in all state and territory education agencies tasked with championing health education best practices, and holding schools accountable for improving student health and well-being); and strengthening certification, professional preparation, and ongoing professional development in health education for teachers at both the elementary and secondary levels. Recommendations also call for stronger alignment and coordination between the public health and education sectors. The committee is now moving ahead on prioritizing the recommendations and developing action steps to address them.
Integrating Youth Health Education and Health Literacy: Success Stories
Minnesota statewide model: integrating school health education and health literacy through broad partnership.
The Roundtable on Health Literacy held a workshop on health literacy and public health in 2014, with examples of how state health departments are addressing health literacy in their states [ 28 ]. One recent example of a strong collaboration between K–12 education and public health agencies is the Statewide Health Improvement Partnership (SHIP) within the Minnesota Department of Health’s Office of Statewide Health Initiative [ 35 ].
SHIP was created by a landmark 2008 Minnesota health reform law. The law was intended to improve the health of Minnesotans by reducing the risk factors that lead to chronic disease. The program funds grantees in all of the state’s 87 counties and 10 tribal nations to support the creation of locally driven policies, systems, and environmental changes to increase health equity, improve access to healthy foods, provide opportunities for physical activity, and ensure a tobacco-free environment [ 35 ]. Local public health agencies collaborate with partners including schools, childcare settings, workplaces, multiunit housing facilities, and health care centers through SHIP.
SHIP models the integration of (1) law, (2) policy, (3) goal setting, and (4) resource building and forging some 2,000 collaborative partnerships and measuring outcomes. SHIP sets a helpful example for others attempting to create synergies across the intersections of state government, health education, local communities, and private organizations. The principles of health literacy are within these collaborations.
Grantees throughout the state have received technical assistance and training to improve school nutrition and physical activity strategies (see Figure 1 ). SHIP grantees and their local school partner sites set goals and adopt best practices for physical education and physical activity inside and outside the classroom. They improve access to healthy food environments through locally sourced produce, lunchrooms with healthier food options, and school-based agriculture. In 2017, SHIP grantees partnered with 995 local schools and accounted for 622 policy, systems, and environmental changes.

SOURCE: Minnesota Department of Health, Office of Statewide Health Improvement Initiatives. 2012. Statewide Health Improvement Partnership Evaluation Data, Minnesota Department of Health Legislative Report 2017. Reported by SHIP grantees using the REDCap system. This data represents the activities and reach of partner sites active between September 24, 2016, and August 25, 2017.
Minnesota has also undertaken a broad approach to health literacy by educating stakeholders and decision makers (i.e., administrators, food service and other staff, students, community partners, and parents) about various health-related social and environmental issues to reduce students’ chronic disease risks.
SHIP grantees assist in either convening or organizing an established school health/wellness council that is required by USDA for each local education agency participating in the National School Lunch Program and/or School Breakfast Program [ 46 , 47 ]. A local school wellness policy is required to address the problem of childhood obesity by focusing on nutrition and physical activity. SHIP also requires schools to complete an assessment that aligns with the WSCC model and provides annual updates. Once the assessment is completed by a broad representation of stakeholders, SHIP grantees assist schools in prioritizing and working toward annual goals. The goal setting and assessment and goal-setting cycle is continuous.
The Bigger Picture: A Case Study of Community Integration of Health Education and Health Literacy
Improving the health literacy of young people not only influences their personal health behaviors but also can influence the health actions of their peers, their families, and their communities. According to the SEARCH for Diabetes in Youth study funded by the CDC and the National Institutes of Health’s National Institute of Diabetes, Digestive, and Kidney Diseases, from 2002 to 2012, the national rate of new diagnosed cases of Type 2 diabetes increased 4.8% [ 32 ]. Among youth ages 10–19, the rate of new diagnosed cases of Type 2 diabetes rose most sharply in Native Americans (8.9%) (although not generalizable to all Native American youth because of small sample size), compared to Asian Americans/Pacific Islanders (8.5%), non-Hispanic blacks (6.3%), Hispanics (3.1%), and non-Hispanic whites (0.6%).
Since 2011, Dean Schillinger, Professor of Medicine in Residence at the University of California San Francisco and Chief of the Diabetes Prevention and Control Program for the California Department of Public Health, has led a capacity-building effort to address Type 2 diabetes [ 23 , 28 , 44 ].
This initiative called The Bigger Picture (TBP) has mobilized collaborators to create resources by and for young adults focused on forestalling and, hopefully, reversing the distressing increase in pediatric Type 2 diabetes by exposing the environmental and social conditions that lead to its spread. Type 2 diabetes is increasingly affecting young people of color, and TBP is specifically developed by and directed to them.
TBP seeks to increase the number of well-informed young people who can participate in determining their own lifelong health behaviors and influencing those of their friends, families, communities, and their own children. The project aims to create a movement that changes the conversation about diabetes from blame- and-shame to the social drivers of the epidemic [ 23 ].
TPB is described by the team that created it as a “counter-marketing campaign using youth-created, spoken-word public services announcements to re-frame the epidemic as a socio-environmental phenomenon requiring communal action, civic engagement, and norm change” [ 44 ]. The research team provides a description of questionnaire responses to nine of the public service announcements in the context of campaign messages, film genre and accompanying youth value, participant understanding of film’s public health message, and the participant’s expression of the public health message. The investigators also correlate the responses with dimensions of health literacy such as conceptual foundations, functional health literacy, interactive health literacy, critical skills, and civic orientation.
One of the campaign partners, Youth Speaks, has created a toolkit to equip and empower students and communities to become change agents in their respective environments, raising their voices and joining the conversation about combating the spread of Type 2 diabetes [ 56 ].
In a discussion of qualitative evaluations of TBP and what low-income youth “see,” Schillinger et al. note that “TBP model is unique in how it nurtures and supports the talent, authenticity, and creativity of new health messengers: youth whose lived experience can be expressed in powerful ways” [ 44 ].
COVID-19: Health Crisis Affecting Children and their Families and a Need for Health Education and Health Literacy in K-12
In a recent op-ed, Rebecca Winthrop, co-director of the Center for Universal Education and Senior Fellow of Global and Economic Development of the Brookings Institution asked, “COVID-19 is a health crisis. So why is health education missing from school work?” [ 58 ] She notes that “helping sustain education amid crises in over 20 countries, I’ve learned that one of the first things you do, after finding creative ways to continue educational activities, is to incorporate life-saving health and safety messages.” Her call is impassioned for age-appropriate, immediately available resources on COVID-19 that can be easily incorporated into distance lesson plans for both children and families. Many organizations, such as Child Trends, are curating collections of such resources. Framing these materials using principles of health literacy and incorporating them into health education messages and resources may be an ideal model for incorporating new pathways for public health K–12 learning.
Call to Action for Collaboration
Strategic and dedicated efforts are needed to bridge health education and health literacy. These efforts would foster the expertise to provide students with the information needed to access and assess useful health information, and to develop the necessary skills for an emerging understanding of health.
Starting with students in school settings, learning to be health literate helps overcome the increased incidence of chronic diseases such as Type 2 diabetes, and imbues a sense of self-efficacy and empowerment through health education. It also sets the course for lifelong habits, skills, and decision making, which can also influence community health.
Pursuing institutional changes to reduce disparities and improve the health of future generations will require significant collaboration and quality improvement among leaders within health education and health literacy. Recommendations provided in previous reports such as IOM’s 1997 report, Schools and Health: Our Nation’s Investment [ 26 ]; the 2004 IOM report on Health Literacy [ 27 ]; and the 2010 National Action Plan to Improve Health Literacy [ 49 ] should be revisited. More recently, a November 2019 Health Literacy Roundtable Workshop (1) explored the necessity of developing health literacy skills in youth, (2) examined the research on developmentally appropriate health literacy milestones and transitions and measuring health literacy in youth, (3) described programs and policies that represent best practices for developing health literacy skills in youth, and (4) explored potential collaborations across disciplines for developing health literacy skills in youth [ 38 ]. With its resulting report, the information provided in the workshop should provide additional insights into collaborations needed to reduce institutional barriers to youth health literacy and empowerment.
At the national level, representatives from public sector health and education levels (e.g., HHS’s Office of Disease Prevention and Health Promotion, CDC, Department of Education) can collaborate with school-based nongovernmental organizations (e.g., SOPHE, ASCD, ASHA, National Association of State Boards of Education, School Superintendents Association, Council of Chief State School Officers, Society of State Leaders of Health and Physical Education) to provide data and lead reform efforts. Leaders of higher education (e.g., Association of American Colleges and Universities, Association of Schools and Programs of Public Health) can join with philanthropies and educational scholars to pursue curricular reforms and needed research to further health education and health literacy as an integral component of higher education.
Among the approaches needed are (1) careful incorporation of key principles of leadership within systems; (2) the training and evaluation of professionals; (3) finding and sharing replicable, effective examples of constructive efforts; and (4) including young people in the development of information and materials to ensure their accessibility, appeal, and utility. Uniting the wisdom, passion, commitment, and vision of the leaders in health literacy and health education, we can forge a path to a healthier generation.
Acknowledgments
The authors would like to express our gratitude to Melissa French and Alexis Wojtowicz for their support in the development of this paper.
Funding Statement
The views expressed in this paper are those of the authors and not necessarily of the authors’ organizations, the National Academy of Medicine (NAM), or the National Academies of Sciences, Engineering, and Medicine (the National Academies). The paper is intended to help inform and stimulate discussion. It is not a report of the NAM or the National Academies.
Conflict-of-Interest Disclosures: Wilma Alvarado-Little has no relevant financial or non-financial relationships to disclose. She contributed to this article based on her experience in the field of health literacy and cultural competency and the opinions and conclusions of the article do not represent the official position of the New York State Department of Health. Cherylee Sherry discloses that she works for the Minnesota Department of Health in the Office of Statewide Health Improvement Initiatives which oversees the Statewide Health Improvement Partnership Program funded by the State of Minnesota.
Contributor Information
M. Elaine Auld, Society for Public Health Education.
Marin P. Allen, National Institutes of Health (ret.)
Cicily Hampton, University of North Carolina at Charlotte.
J. Henry Montes, American Public Health Association.
Cherylee Sherry, Minnesota Department of Health.
Angela D. Mickalide, American College of Preventive Medicine.
Robert A. Logan, U.S. National Library of Medicine and University of Missouri-Columbia.
Wilma Alvarado-Little, New York State Department of Health.
Kim Parson, KPCG, LLC.
- Entertainment
- Environment
- Information Science and Technology
- Social Issues
Home Essay Samples
Essay Samples on Health
The healthcare college majors belong to those students that have to compose a great number of essays that include reflective journals, shadowing experience reports, lab analysis explorations, argumentative papers, and assignments on theorists. Since these are quite complex, it’s important to know the difference between these essay types. You should check twice with your grading rubric and always ask questions if you are in doubt. As a way to provide you with some guidance, we have compiled a collection of free health essay examples. These focus on various branches of nursing, healthcare administration, pharmacology, international issues, and the basic health subjects that every medical student may face. Take your time to analyze at least five health essay samples by starting with the introduction section. Your first essay paragraph must provide information about the problem before coming up with your thesis statement. Remember that you should have at least five reliable sources that support your argument or the basic facts that you may require for debates. Speaking of medical lab reports, you can use various assignments below as a template that will help you structure your health paper. Take your time to explore free samples and it will always pay off!
Unveiling My Career Goals in the Healthcare Field
What are your career goals related to the healthcare field? This question unveils my aspirations to contribute to the well-being of individuals, families, and communities by venturing into the dynamic and impactful realm of healthcare. A career in healthcare is not only a path to...
- Career Goals
- Health Care
The Nursing Discourse Community: Shared Knowledge and Collaboration
Nursing is a noble and demanding profession that thrives on collaboration, empathy, and the exchange of knowledge. Within the vast healthcare landscape, the concept of a nursing discourse community emerges as a dynamic network of professionals who share a common language, values, and goals. This...
- Discourse Community
Pursuing Public Health: Navigating a Path to Achieve Career Goals
Public health career goals reflect the aspirations of individuals committed to safeguarding and improving the well-being of communities on a large scale. In a world where health challenges are diverse and ever-evolving, a career in public health offers a unique opportunity to make a lasting...
- Public Health
How Does Community Influence You: Shaping Identity, Values
How does community influence you? This question delves into the multifaceted impact that the communities we are a part of have on shaping our identity, values, aspirations, and the lens through which we perceive the world. Whether we realize it or not, the influence of...
- Under The Influence
Effects of Drugs on Community: Unraveling the Impact
The effects of drugs on community are far-reaching and profound, touching every aspect of society. This essay explores the significance of drug-related issues, the multifaceted impact on communities, the challenges they pose, and the importance of collaborative efforts to mitigate the harm caused by drugs....
Stressed out with your paper?
Consider using writing assistance:
- 100% unique papers
- 3 hrs deadline option
Community Health Nursing: Bridging Care and Empowerment
Community health nursing is a vital branch of nursing that plays a pivotal role in promoting the well-being of individuals, families, and communities at large. This essay delves into the significance of community health nursing, its core principles, the role of community health nurses, and...
My Future Career as a Nurse: Way for Compassionate Healing
The journey toward a future career as a nurse is one that intertwines empathy, expertise, and the unwavering commitment to provide compassionate care. In this essay, I take you on a voyage through my aspirations, motivations, and the profound impact I intend to make as...
What Motivates You to Pursue a Career in Medicine
The world of medicine is a tapestry of compassion, science, and unwavering commitment. In this essay, we embark on an exploration of the question: what motivates you to pursue a career in medicine? By delving into the layers of empathy, fascination, and the desire to...
Why You Choose Nursing as a Career: A Comprehensive Analysis
The decision to pursue a nursing career is often rooted in profound motivations and a desire to make a meaningful impact on the lives of others. In this essay, we embark on a thorough analysis of why individuals choose nursing as a career, exploring the...
Cell Phone Addiction: Unraveling the Digital Dilemma
In the modern age of technology, cell phones have become an integral part of our lives, offering convenience, connectivity, and access to a world of information at our fingertips. However, the rapid proliferation of cell phones has given rise to a concerning phenomenon: cell phone...
- Cell Phones
Why Smoking is "Good" for You: Unraveling the Enigma
The Complex Landscape of Smoking: An Exploration Observing the individual engrossed in his smoke, one can't help but notice the allocated space designated exclusively for smokers. Evidently, his financial prosperity allows him to indulge in this habit, as smoking tends to be associated with those...
- Tobacco Use
Why Should We Legalize Abortion: Empowering Women's Choice and Safety
The debate over legalizing abortion has been a subject of intense discussion and controversy for decades. In this essay, we will explore the compelling reasons why many advocate for the legalization of abortion, focusing on the importance of women's rights, public health, and the reduction...
- Pro Choice (Abortion)
Why Should Abortions Be Made Legal: Advancing Women's Rights
The topic of why should abortions be made legal has sparked heated debates around the world. In this essay, we will delve into the compelling reasons why abortion should be legal, highlighting the importance of women's rights, public health, and the avoidance of unsafe practices....
- Women's Rights
Why I Agree: Abortion from a Supportive Perspective
This essay focuses on arguments in favor of abortion, highlighting reproductive rights, autonomy, health considerations, and societal benefits. Introduction Abortion is a topic that has sparked intense debate and has led to differing viewpoints across societies. This essay takes a stance in favor of abortion,...
- Reproductive Rights
Why Abortion Should Not Be Banned: Preserving Choice
The debate over whether abortion should be banned is a deeply complex and emotionally charged one. In this essay, we will explore the reasons why many argue against banning abortion, highlighting the importance of women's rights, healthcare access, and the potential consequences of prohibition. By...
The Life of a Doctor: Challenges, Commitment, and Compassion
This essay delves into the multifaceted life of a doctor, exploring the demands of their profession, the impact they have on patients and communities, and the personal fulfillment that comes from their vocation. Introduction The life of a doctor is often revered and admired, symbolizing...
The Importance of Doctors: Nurturing Health and Healing
This essay highlights the significance of doctors in society as healers, innovators, advocates, and compassionate caregivers. Doctors play a crucial role in diagnosing and treating diseases, preventing health issues, leading medical advancements, advocating for public health, and nurturing human connections. Their contributions extend far beyond...
The Evolution and Controversy of Abortion Laws
Abortion laws have long been a source of contentious debate around the world, reflecting the complex interplay of cultural, religious, ethical, and political factors. This essay delves into the historical evolution of abortion laws, examines the diverse legal approaches taken by different countries, and explores...
- Controversial Issue
The Controversy Surrounding Abortion Rights
The issue of abortion rights is one of the most contentious debates in modern society, touching upon deeply held beliefs about women's autonomy, morality, and the role of government in personal decisions. This essay seeks to provide an in-depth analysis of abortion rights, examining the...
The Case for Legal Abortion: Balancing Women's Rights and Health
The question of whether abortion should be legal is a subject of profound ethical, medical, and social importance. In this argumentative essay, we will explore the reasons why many advocate for legalizing abortion, highlighting the importance of women's rights, access to safe medical procedures, and...
The Argumentative Discourse About the Legalization of Abortion
The topic of the legalization of abortion has ignited passionate and contentious debates worldwide, touching on issues of ethics, women's rights, healthcare, and government intervention. This essay delves into the argumentative discourse surrounding the legalization of abortion, exploring its ethical implications, women's agency, healthcare access,...
The Argumentative Case for Legalizing Abortion
The contentious topic of legalizing abortion has been at the center of heated debates for decades, drawing on a multitude of ethical, societal, and personal considerations. In this argumentative essay, we delve into the rationale behind legalizing abortion, highlighting how it empowers women's autonomy, safeguards...
The Argument for Legalizing Abortion: Safety and Reproductive Rights
Introduction The debate surrounding the legalization of abortion is a contentious and complex issue that touches upon ethics, women's rights, and societal norms. This essay aims to present a comprehensive argument in favor of legalizing abortion, highlighting the importance of empowerment, safety, and reproductive rights...
The Abortion Proposal: A Constructive Approach to a Polarizing Issue
Introduction Abortion remains one of the most divisive topics in many societies, consistently sparking passionate debates. The complexities surrounding the issue necessitate an approach that transcends political, religious, and cultural lines. This abortion proposal essay seeks to outline a multi-faceted strategy that combines education, access...
The Abortion Problem: A Deep Dive into Its Complexities
Introduction The abortion problem has been a matter of intense debate for centuries. This complex issue intertwines medical, ethical, cultural, and political facets. As societies have evolved, so have the perceptions and policies regarding abortion. The discussions often diverge into two primary perspectives: pro-choice, emphasizing...
- Social Problems
The Abortion Issue: Exploring Diverse Perspectives
The abortion issue remains one of the most contentious and emotionally charged debates in modern society. This essay aims to provide a comprehensive overview of the multifaceted aspects surrounding the abortion issue, examining the historical, legal, ethical, and societal dimensions that shape individual viewpoints and...
- Pro Life (Abortion)
The Abortion Discussion: Diverse Perspectives and Complex Considerations
Introduction The abortion discussion is a contentious and deeply nuanced discourse that engages individuals, communities, policymakers, and societies across the globe. This essay aims to delve into the multifaceted dimensions of the abortion discussion, considering the range of perspectives, ethical considerations, legal frameworks, and societal...
The Abortion Debate: Exploring Both Sides of the Argument
Introduction The issue of abortion has long been a topic of fervent debate, stirring impassioned arguments from various corners of society. This essay aims to provide a comprehensive examination of the arguments on both sides of the abortion debate. By delving into the viewpoints of...
- Abortion Debate
The Abortion Controversy: Navigating Complex Ethical Arguments
Introduction The abortion controversy stands as one of the most polarizing and emotionally charged debates in society. This abortion controversial argumentative essay seeks to delve into the multifaceted dimensions of the abortion controversy, analyzing the diverse arguments and perspectives that shape this ongoing discourse. The...
- Ethical Dilemma
Teenage Pregnancy and Abortion: Navigating Complex Choices
The issue of teenage pregnancy and abortion is a multifaceted topic that intersects with issues of sexuality, education, health, and personal choices. In this essay, we will explore the challenges posed by teenage pregnancy, the implications of abortion for young women, and the importance of...
- Teenage Pregnancy
Supporting Abortion: Empowering Women's Rights and Health
The issue of abortion is a topic that invokes a range of emotions and opinions. In this essay, we will delve into the reasons for supporting abortion, emphasizing the importance of women's rights, bodily autonomy, and the advancement of public health. By exploring these facets,...
Should Abortion Be Made Legal? A Comprehensive Examination
The question of whether abortion should be made legal is a deeply divisive and complex issue that elicits passionate arguments from individuals on both sides of the debate. This essay aims to explore the arguments for and against legalizing abortion, considering a range of ethical,...
Should Abortion Be Legalized? Argument for Reproductive Freedom
This essay presents a comprehensive argument in favor of legalizing abortion, focusing on reproductive freedom, women's health, and societal impact. Introduction The question of whether abortion should be legalized is a topic that generates intense debates worldwide. This essay aims to provide a comprehensive examination...
Should Abortion be Legal or Illegal: Legalization vs. Criminalization
The question of whether abortion should be legal or illegal is at the heart of a contentious and deeply complex debate. In this argumentative essay, we will examine the merits and drawbacks of both sides of the argument, exploring the ethical, medical, and societal considerations...
Should Abortion Be Illegal? The Controversial Debate
The question of whether abortion should be illegal is a contentious and morally charged issue that revolves around conflicting beliefs about the value of life, women's rights, and societal well-being. In this argumentative essay, we will explore the reasons why some argue that abortion should...
Roe vs. Wade and the Abortion Debate
The landmark Supreme Court case of Roe v. Wade in 1973 marked a pivotal moment in the ongoing abortion debate, shaping the legal landscape surrounding reproductive rights in the United States. This essay examines the Roe v. Wade decision, delving into its historical context, ethical...
Research about Abortion: The Complex Landscape
The topic of abortion is one that elicits passionate debates and encompasses a myriad of ethical, medical, social, and legal dimensions. In this research essay, we will delve into the multifaceted nature of abortion, exploring its historical context, ethical considerations, medical practices, legal frameworks, and...
Reasons Why Abortion Should Be Legalized: A Comprehensive Exploration
The debate over whether abortion should be legalized is a complex and contentious issue, raising ethical, medical, and societal considerations. In this essay, we will delve into the compelling reasons why abortion should be legalized, focusing on the importance of women's autonomy, safeguarding public health,...
Reasons Abortion Should Be Legal
The question of whether abortion should be legal is a deeply divisive and complex issue, intertwining ethical, medical, and societal factors. In this essay, we will delve into the compelling reasons why abortion should be legal, focusing on the ethical importance of women's autonomy, public...
Persuasive Writing: The Imperative of Legal Abortion
The topic of legal abortion has been a point of intense contention, evoking impassioned debates on ethics, women's rights, and the role of government in personal decisions. In this essay, we will explore the compelling reasons why legal abortion is not only a necessity but...
Navigating the Complex Issue of Abortion: Ethics, Rights, and Choices
The issue of abortion has long been a subject of profound ethical, legal, and social debate, spanning cultural, religious, and philosophical landscapes. With divergent perspectives and deeply held beliefs, this complex issue encompasses questions about the sanctity of life, individual autonomy, medical ethics, and the...
Is Abortion Morally Wrong? Unpacking Moral Perspectives
The moral status of abortion has long been a contentious and complex issue, eliciting impassioned debates that touch on ethics, religion, philosophy, and individual beliefs. The question of whether abortion is morally wrong stands at the heart of these discussions, prompting diverse viewpoints and thought-provoking...
Is Abortion Morally Right? Exploring the Moral Dilemma
Abortion has been a topic of intense ethical and moral debate for decades, sparking discussions on the rights of women, the sanctity of life, and the role of government in personal decisions. The question of whether abortion is morally right elicits strong opinions from individuals...
In Defense of Abortion: Exploring the Argument for Reproductive Rights
The essay presents a comprehensive argument in favor of abortion, focusing on reproductive rights, women's autonomy, and the complexities of individual circumstances. Introduction The topic of abortion is one of the most debated and controversial issues in society. This essay seeks to present a strong...
How Do You Show Empathy to Patients: The Heartfelt Approach
**How do you show empathy to patients?** This question lies at the core of providing patient-centered care that goes beyond medical treatment to touch the realms of emotional support and understanding. Empathy is the art of connecting with patients on a human level, acknowledging their...
For Abortion: An Argumentative Analysis
The issue of abortion has been a subject of intense controversy and debate for decades, with individuals and societies holding contrasting viewpoints on its moral, ethical, and legal implications. This argumentative essay aims to explore the various perspectives surrounding abortion, delving into the arguments both...
Exploring the Anti-Abortion Perspective: Values and Ethics
Introduction The topic of abortion has long been a contentious and deeply divisive issue, sparking intense debates worldwide. This essay delves into the anti-abortion perspective, also known as the pro-life stance, which emphasizes the sanctity of human life from conception and opposes the practice of...
Exploring Abortion Solutions: A Comprehensive Examination
Introduction The complex issue of abortion prompts a search for practical and ethical solutions that balance women's rights, societal values, and the well-being of all involved. This essay delves into a range of abortion solutions, exploring approaches that address the diverse challenges surrounding this contentious...
Empowering Choice and Advancing Women's Health
The topic of abortion remains a subject of impassioned discourse, with diverse viewpoints rooted in ethics, religion, personal beliefs, and women's rights. In this persuasive essay, we will explore the critical arguments in favor of legalizing abortion, focusing on how it empowers women's agency, protects...
Disadvantages of Abortion: Navigating Ethical and Emotional Challenges
Introduction The topic of abortion is a contentious and emotionally charged subject that sparks debates around the world. While discussions about abortion often focus on individual rights, women's health, and legal considerations, it's crucial to also explore the disadvantages associated with this complex decision. This...
Arguments Against Abortion: The Ethical and Moral Debate
The topic of abortion has long been a subject of passionate debate, with opinions ranging from staunch support to vehement opposition. This essay will delve into the arguments against abortion, exploring the ethical, moral, and religious perspectives that contribute to this contentious issue. The Sanctity...
Anti-Abortion Argument: Protecting Life and Ethical Considerations
Introduction The debate over abortion is characterized by deeply held beliefs and passionate arguments from both sides. This essay delves into the anti-abortion argument, also known as the pro-life stance, which asserts that the fetus has a right to life and should be protected from...
Agreeing with Abortion: Upholding Reproductive Rights and Autonomy
Introduction The topic of abortion is marked by passionate debates, with various perspectives and viewpoints coming to the forefront. This essay explores the arguments in favor of abortion, specifically focusing on the principles of reproductive rights, bodily autonomy, and the importance of providing individuals with...
Agree with Abortion: Exploring the Rationale and Ethical Perspectives
This essay has explored the rationale behind agreeing with abortion, shedding light on the ethical and contextual factors that contribute to this perspective. While the topic of abortion remains contentious, understanding the arguments of those who support it is essential for engaging in informed and...
Agree to Abortion: Exploring a Pro-Choice Perspective
Introduction The topic of abortion has been a subject of intense debate, sparking impassioned arguments from both proponents and opponents. This essay delves into the reasons and arguments for agreeing with the practice of abortion, focusing on women's autonomy, reproductive rights, and the complex circumstances...
Against Abortion: Examining the Argument for Protecting Fetal Life
The essay presents a comprehensive argument against abortion, focusing on fetal rights, ethical considerations, and alternatives to abortion. Introduction The debate surrounding abortion is one that elicits strong emotions and differing viewpoints. This essay delves into the argument against abortion, also known as the pro-life...
Against Abortion: Examining Ethical Concerns
Introduction The issue of abortion has long been a subject of intense debate, with passionate arguments on both sides. This essay delves into the arguments against abortion, focusing on ethical concerns and moral perspectives that drive opposition to this practice. By analyzing the sanctity of...
Against Abortion: Examining Ethical and Moral Considerations
Introduction The topic of abortion is inherently complex and evokes strong emotions from various perspectives. This essay delves into the arguments against abortion, focusing on ethical and moral considerations that underlie the opposition to this practice. It acknowledges the nuanced nature of this issue and...
Against Abortion Persuasive Arguments: Voicing Opposition
Introduction The topic of abortion is one that evokes strong emotions and polarizing opinions. In this persuasive essay, we will delve into the reasons why one might take a stance against abortion. By exploring the sanctity of life, the potential for alternatives, and the potential...
Advantages of Abortion: Exploring Benefits and Complexities
Introduction The topic of abortion is one of the most contentious issues in society, sparking debates and discussions on ethics, morality, and women's rights. While the debate often focuses on the disadvantages and challenges associated with abortion, it's important to also consider the potential advantages...
Advantages and Disadvantages of Abortion: Weighing the Pros and Cons
Introduction The topic of abortion is a complex and sensitive issue that elicits strong opinions from individuals across the globe. While the debate often centers around the ethical, moral, and legal aspects of abortion, it's important to consider both the advantages and disadvantages associated with...
About Abortion: Exploring a Complex Topic
Introduction Abortion is a complex and contentious topic that elicits strong emotions and differing viewpoints. It revolves around the termination of a pregnancy, raising significant ethical, legal, and societal questions. This essay provides an overview of abortion, exploring its history, methods, legal status, and the...
Abortion: Navigating the Ethical and Personal Choice
The topic of abortion is an ethical and emotional minefield that sparks passionate debates on both sides. The central issue revolves around a woman's right to choose and the moral status of the unborn fetus. This short argumentative essay will delve into the key points...
Abortion: Navigating Complex Choices in 1000 Words
Introduction The topic of abortion is both intricate and polarizing, encompassing a multitude of moral, ethical, legal, and personal considerations. This essay will explore the various dimensions of abortion, ranging from its historical context to the current debates surrounding it. While no concise essay can...
Abortion: Arguments For and Against
The topic of abortion is one that elicits strong opinions and impassioned debates. While some individuals firmly believe in a woman's right to choose, others advocate for the sanctity of unborn life. This essay will examine the arguments both for and against abortion, highlighting the...
Abortion: An Examination of Yes and No Arguments
Introduction The debate over abortion has polarized societies, sparking impassioned arguments from both proponents and opponents. This essay delves into the arguments for and against abortion, exploring the complexities and ethical considerations that underlie the "yes" and "no" perspectives on this divisive issue. Proponents of...
Abortion: An Argumentative Examination of a Complex Issue
The topic of abortion is a contentious and deeply divisive subject that elicits strong emotions and stirs heated debates. At the heart of this issue lies the clash between the right to bodily autonomy and the sanctity of life. This essay seeks to provide an...
Abortion: A Complex and Controversial Issue in 500 Words
Abortion, the termination of a pregnancy, is a deeply divisive topic that elicits strong emotions and diverse perspectives. The controversy surrounding abortion arises from the collision of moral, ethical, religious, and societal values, making it one of the most complex issues in contemporary discourse. The...
Abortion Should Not Be Banned
Introduction The topic of abortion is one of deep ethical, moral, and societal significance. The question of whether abortions should be banned is a highly debated issue, with differing perspectives on both sides. This essay argues that abortion should not be banned, highlighting the importance...
Abortion Should Be Legal: An Argumentative Perspective
Introduction The legalization of abortion is a deeply polarizing issue that sparks debates encompassing ethics, human rights, women's autonomy, and societal well-being. This essay presents a comprehensive argument in favor of legalizing abortion, addressing both the practical and moral considerations surrounding this complex topic. Historical...
Abortion Should Be Legal: A Persuasive Argument
Introduction The topic of abortion has long been a subject of heated debate, sparking conversations about ethics, women's rights, and societal values. This persuasive essay aims to present a compelling case for the legalization of abortion, highlighting the importance of respecting women's autonomy, safeguarding their...
Abortion Should Be Allowed: Ensuring Women's Autonomy and Health
Introduction The question of whether abortion should be allowed is a complex and highly debated topic that revolves around women's rights, medical ethics, and societal values. This essay argues in favor of allowing abortion, highlighting the importance of women's autonomy over their bodies, protecting their...
Abortion Rights: Complexities of an Argumentative Landscape
Introduction The debate over abortion rights remains one of the most contentious and emotionally charged issues in modern society. The clash of ideologies and moral beliefs has led to a multifaceted discussion that touches upon ethical, legal, religious, and personal considerations. The focus of this...
Abortion Rights: Balancing Autonomy and Ethics
Introduction Abortion rights, the subject of ongoing debates, involve the intersection of women's autonomy, medical ethics, and societal values. This essay explores the complexities surrounding abortion rights, delving into the historical, legal, ethical, and social dimensions that shape this contentious issue. Historical Evolution The history...
Abortion Legalization: Examining the Complex Issue
The legalization of abortion is a topic that evokes strong emotions and opinions from individuals on all sides of the debate. This essay delves into the multifaceted discussions surrounding the legalization of abortion, exploring the arguments presented by proponents and opponents and the broader implications...
Abortion Laws and Reproductive Rights: Argumentative Debate
The issue of abortion laws has been a hotly debated topic that touches on ethical, moral, and legal considerations. This argumentative essay explores the opposing viewpoints surrounding abortion laws and the broader implications for reproductive rights and women's autonomy. Proponents of Restrictive Abortion Laws Advocates...
Abortion Information: Exploring the Complexities and Perspectives
Abortion is a deeply contentious and multifaceted topic that touches upon matters of ethics, human rights, public health, and personal beliefs. This informative essay aims to provide a comprehensive overview of abortion, shedding light on its historical context, legal landscape, medical procedures, and the various...
Abortion in America: A Complex and Controversial Issue
The topic of abortion in America is one that remains deeply divisive and emotionally charged. As a fundamental issue of women's rights, personal choice, and ethical considerations, the debate over abortion laws and access continues to shape the social, political, and legal landscape of the...
Abortion Facts for an Argument
Abortion is a complex and emotionally charged topic that elicits strong opinions from individuals across society. When constructing an argumentative essay on abortion, it is essential to base your points on accurate and well-researched facts. Here are several key abortion facts that can serve as...
Abortion Disagree: Ethical Concerns and Alternative Perspective
Introduction The topic of abortion is a highly contentious and morally complex issue that evokes deeply-held beliefs and diverse perspectives. This "Abortion Disagree" essay aims to present arguments against abortion by exploring the ethical concerns and alternative viewpoints held by those who do not agree...
Abortion as a Social Issue: Navigating Perspectives and Impacts
Introduction Abortion is a multifaceted social issue that intertwines ethics, women's rights, religion, public health, and societal values. This essay delves into the complexities surrounding abortion as a social issue, exploring its historical context, the diverse viewpoints it elicits, and the broader implications for individuals...
Abortion Argumentative: Navigating the Complex Ethical Debate
Introduction The topic of abortion is a deeply contentious and ethically charged subject that has sparked heated debates for years. This abortion argumentative essay aims to provide an in-depth analysis of the complex ethical considerations surrounding abortion. The discourse on abortion is multifaceted, involving discussions...
Abortion and the Moral Debate: Is It Murder?
The topic of abortion sparks intense moral and ethical debates, with one of the central questions being whether abortion can be equated with murder. This essay aims to delve into the complexities of this debate, examining the perspectives of both pro-life advocates who contend that...
Abortion and Philosophy: Navigating Ethical and Moral Dimensions
The topic of abortion is a philosophical dilemma that challenges individuals to grapple with complex ethical and moral questions. This essay delves into the philosophical underpinnings of the abortion debate, examining the various perspectives and philosophical arguments that contribute to the discourse. The Moral Status...
- Personal Philosophy
Abortion and Euthanasia: Ethical and Moral Dilemmas
Introduction The ethical debates surrounding abortion and euthanasia are among the most contentious and complex issues in contemporary society. Both topics touch on deeply personal and profound matters related to life, death, autonomy, and the value of human existence. This essay delves into the ethical...
Abortion Analysis: Exploring Complex Factors and Perspectives
Introduction The topic of abortion is a deeply complex and emotionally charged issue that spans medical, ethical, legal, and social domains. This essay undertakes a comprehensive abortion analysis, delving into the various factors, perspectives, and considerations that contribute to the ongoing debate surrounding this sensitive...
Abortion Advantages: Empowering Reproductive Autonomy
Introduction The topic of abortion is deeply nuanced, encompassing a range of perspectives and considerations. This essay explores the advantages of abortion, emphasizing the importance of reproductive autonomy, individual well-being, and the empowerment of women in making decisions about their bodies and futures. Reproductive Autonomy...
Abortion Advantages and Disadvantages: Weighing the Complexities
Introduction The topic of abortion is fraught with ethical, social, and personal considerations, making it a subject of ongoing debate and reflection. This essay delves into the advantages and disadvantages of abortion, shedding light on the complex factors that individuals and societies must grapple with...
A Visit to the Doctor: Navigating Care and Wellness
This essay has explored the various aspects of a visit to the doctor, highlighting its significance in navigating care and wellness. From the decision to seek medical attention to the interactions with healthcare professionals, a visit to the doctor is a pivotal step in the...
A Thoughtful Speech about Abortion: Exploring Diverse Perspectives
Ladies and gentlemen, esteemed guests, and fellow citizens, today we gather to delve into one of the most complex and emotionally charged topics of our time: abortion. The issue of abortion is marked by strong convictions and divergent viewpoints, and as we engage in this...
Why I Am Thankful for My Health: Celebrating Well-Being
My health is a precious gift that allows me to live life to the fullest, pursue my passions, and experience the world's wonders. Each day of well-being is a reminder of the importance of taking care of myself and cherishing the vitality that enables me...
Why Healthcare Should Not Be Free
The debate over healthcare reform has sparked discussions about the best way to ensure access to medical services for all individuals. While the idea of free healthcare may seem appealing on the surface, a closer examination reveals potential drawbacks that must be considered. This essay...
Why Birth Control Should Be Free: A Step Towards Progress
Access to affordable healthcare is a fundamental human right, and within that scope, access to contraception and birth control is equally crucial. The debate over whether birth control should be freely accessible has been ongoing for years. In this essay, we will delve into the...
- Birth Control
Unraveling the Factors: Exploring Causes of Mental Illness in Youth
Mental illness among youth has become an increasingly pressing concern in today's society. Adolescence is a critical developmental period characterized by significant changes in emotions, behaviors, and social interactions. This essay delves into the complex web of the causes of mental illness in youth, including...
- Mental Illness
The Impact of COVID-19 on Education: An Unprecedented Challenge
Over the past few years, the world has experienced a transformative event that has disrupted every aspect of human life. The COVID-19 pandemic, caused by the novel coronavirus, has left an indelible mark on societies across the globe. One of the most profound areas affected...
The Foundation of Well-Being: Exploring the Importance of Mental Health
In the pursuit of a fulfilling and balanced life, one aspect often overlooked is mental health. Just as physical health is crucial for our well-being, our mental well-being is equally essential. This essay delves into the significance of mental health, its impact on various aspects...
- Mental Health
The Effects of Not Getting Enough Sleep
Sleep is a fundamental aspect of human well-being, yet the modern world often places demands on individuals that can lead to inadequate sleep. The effects of not getting enough sleep are far-reaching and impact various aspects of physical, mental, and emotional health. In this essay,...
- Sleep Deprivation
- Sleep Disorders
The Art of Caring in Nursing and Its Impact on Patients
Nursing is often described as both a science and an art. While the scientific aspect involves medical knowledge and technical skills, the heart of nursing lies in the art of caring. The art of caring goes beyond the application of treatments and medications; it encompasses...
- Nursing Care Plan
Nursing Student's Reflection on Clinical Experience
Stepping into the world of clinical practice as a nursing student was both exhilarating and nerve-wracking. The opportunity to apply classroom knowledge to real patients brought a newfound sense of purpose and responsibility. In this essay, I will reflect on my clinical experience as a...
Is Healthcare a Basic Human Right: Exploring the Complex Issue
Access to healthcare is a fundamental concern that touches upon the well-being and dignity of individuals. The question of whether healthcare is a basic human right is a topic of ongoing debate and has significant implications for society. In this essay, we will explore arguments...
- Human Rights
Best topics on Health
1. Unveiling My Career Goals in the Healthcare Field
2. The Nursing Discourse Community: Shared Knowledge and Collaboration
3. Pursuing Public Health: Navigating a Path to Achieve Career Goals
4. How Does Community Influence You: Shaping Identity, Values
5. Effects of Drugs on Community: Unraveling the Impact
6. Community Health Nursing: Bridging Care and Empowerment
7. My Future Career as a Nurse: Way for Compassionate Healing
8. What Motivates You to Pursue a Career in Medicine
9. Why You Choose Nursing as a Career: A Comprehensive Analysis
10. Cell Phone Addiction: Unraveling the Digital Dilemma
11. Why Smoking is “Good” for You: Unraveling the Enigma
12. Why Should We Legalize Abortion: Empowering Women’s Choice and Safety
13. Why Should Abortions Be Made Legal: Advancing Women’s Rights
14. Why I Agree: Abortion from a Supportive Perspective
15. Why Abortion Should Not Be Banned: Preserving Choice
Need writing help?
You can always rely on us no matter what type of paper you need
*No hidden charges
100% Unique Essays
Absolutely Confidential
Money Back Guarantee
By clicking “Send Essay”, you agree to our Terms of service and Privacy statement. We will occasionally send you account related emails
You can also get a UNIQUE essay on this or any other topic
Thank you! We’ll contact you as soon as possible.
Essay on Health Awareness
Students are often asked to write an essay on Health Awareness in their schools and colleges. And if you’re also looking for the same, we have created 100-word, 250-word, and 500-word essays on the topic.
Let’s take a look…
100 Words Essay on Health Awareness
Understanding health awareness.
Health awareness is about knowing and understanding health issues. It’s like learning about different diseases, their causes, and how to avoid them. Health awareness helps us make better choices for a healthier life.
Importance of Health Awareness
Health awareness is important because it can save lives. It helps us know what’s good and bad for our health. With this knowledge, we can avoid harmful habits like smoking and eating junk food, and adopt healthy habits like exercising and eating balanced meals.
Health Awareness and Disease Prevention
Health awareness helps in preventing diseases. It tells us about vaccines and regular check-ups that help catch diseases early. Also, it teaches us about hygiene practices like washing hands to prevent disease spread.
Role of Schools in Health Awareness
Schools play a big role in health awareness. They teach students about nutrition, physical education, and hygiene. Schools also organize health camps and invite doctors to talk about different health topics.
Also check:
250 Words Essay on Health Awareness
What is health awareness.
Health awareness is about knowing and understanding health issues. It helps us make the right choices for our health. It is about learning how to stay fit, eat right, and take care of our bodies.
Why is Health Awareness Important?
Being aware of health is important for many reasons. It helps us live longer and better lives. When we know about health issues, we can prevent them. For example, knowing that smoking is bad for our lungs can stop us from starting to smoke.
How Can We Improve Health Awareness?
There are many ways to improve health awareness. We can read books, watch videos, or talk to doctors. Schools can also help by teaching students about health. Parents can set a good example by eating healthy food and exercising regularly.
Role of Media in Health Awareness
Media plays a big role in health awareness. TV shows, news, and social media can spread information about health. They can tell us about new research or health risks. But, we must be careful to check if the information is correct. Not all information on the internet is true.
500 Words Essay on Health Awareness
Health awareness is knowing about the state of your body, how to keep it healthy, and what can harm it. It is like a guide to help you live a healthy life. It tells you about good habits like eating right, exercising, and getting enough sleep. It also warns you about bad things like smoking, drinking too much alcohol, or not getting enough exercise.
Health awareness is very important for everyone. It helps you stay healthy and avoid diseases. If you are aware of your health, you can take steps to prevent illness. For example, if you know that eating too much sugar can lead to diabetes, you can choose to eat less sugar. This can help you avoid getting diabetes in the future.
Ways to Increase Health Awareness
There are many ways to increase health awareness. One way is to learn about health from reliable sources. You can read books, watch videos, or talk to health professionals like doctors and nurses. You can also learn about health in school or at health awareness events.
Another way to increase health awareness is to practice healthy habits. This means eating a balanced diet, exercising regularly, getting enough sleep, and avoiding harmful substances like tobacco and alcohol. By doing these things, you can improve your health and learn more about how your body works.
Schools also organize health awareness events. These events can include health fairs, where students can learn about different health topics and get free health screenings. They can also include campaigns to promote healthy habits, like eating fruits and vegetables or walking to school.
In conclusion, health awareness is very important. It helps us stay healthy and avoid diseases. We can increase our health awareness by learning about health and practicing healthy habits. Schools play a big role in health awareness by teaching students about health and organizing health awareness events. By being aware of our health, we can live healthier, happier lives.
That’s it! I hope the essay helped you.
If you’re looking for more, here are essays on other interesting topics:
Happy studying!
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Essay On Health Education
Table of Contents
Short Essay On Health Education
Health education is a crucial aspect of overall health and wellness, as it plays a vital role in helping individuals make informed decisions about their health and well-being. Health education can encompass a range of topics, including personal health, nutrition, physical activity, disease prevention, and healthy lifestyles.
One of the main goals of health education is to empower individuals to take control of their own health. By providing information and resources, health education can help individuals understand the factors that contribute to their health and how they can make positive changes to improve their health and well-being. This can include things like making healthy food choices, engaging in physical activity, managing stress, and avoiding harmful habits like smoking or excessive drinking.
Another important aspect of health education is disease prevention. By providing information about the causes and risk factors for different diseases, health education can help individuals take steps to reduce their risk of developing these conditions. For example, education about the dangers of smoking can help individuals avoid taking up this habit, and education about the importance of getting regular check-ups and screenings can help individuals catch and treat health problems early, before they become more serious.
Health education can also help to reduce health disparities and improve health outcomes for vulnerable populations. For example, health education programs aimed at low-income communities can help individuals understand the importance of healthy lifestyle choices and provide resources and support to help them make positive changes.
In addition to individual health, health education can also contribute to the overall health and well-being of communities and societies. For example, education about the importance of vaccination can help to prevent the spread of disease and protect public health, and education about environmental health can help individuals understand how their actions can impact the environment and the health of their communities.
In conclusion, health education is an essential component of overall health and wellness. By providing individuals with the information and resources they need to make informed decisions about their health, health education can help to empower individuals, reduce health disparities, and improve health outcomes for individuals and communities.
Long Essay On Health Education
Health education is an important part of any country’s health care system. It is responsible for informing the public about health risks and educating them on how to maintain their health. This article will discuss the importance of health education and some methods that can be used to improve it.
What is Health Education?
Health education is the process of teaching people about their health and how to protect it. Health education can take many different forms, from teaching people about diseases and health risks to providing information on healthy eating and lifestyles.
Health education is important because it helps people stay healthy and avoid dangerous conditions. It can also help people get the care they need if they are sick or injured.
There are many ways to deliver health education. Some schools, clinics, and hospitals offer classes specifically focused on health topics. Others provide general education about all aspects of life, including health, in addition to specific programming about health concerns.
health education.
Types of Health Education
There are many different types of health education, but they all share one common goal: to help people be healthier. Some types of health education teach people how to prevent diseases and maintain good health. Other types of health education focus on helping people who have already been diagnosed with a disease or condition.
One type of health education that is particularly important for young people is sexual health education. This type of education teaches kids about sex, birth control, and other related topics. It’s important for kids to learn these things because they may someday want to have a sexual relationship and get pregnant.
Another type of health education that is important for adults is prevention education. Prevention education teaches people how to stay healthy by avoiding risky behaviors. This type of education can help reduce the number of cases of some diseases, such as cancer.
Purpose of Health Education
Health education is an important part of ensuring that all individuals have access to the necessary information and resources to maintain good health. It can also help prevent disease and promote healthy lifestyles. Health educators use a variety of methods to teach people about health and how to maintain it. Some common methods include lectures, group discussions, demonstrations, and curricula.
One of the most important aspects of health education is providing people with accurate information. Health educators must be able to understand complex medical terminology andscience in order to provide accurate information. They must also be able to present this information in a way that is easy for people to understand. In addition, health educators should be able to adapt their teaching styleto match the audience they are addressing.
Health education can also help individuals make informed choices about their own health care. Education can help people better understand the risks and benefits associated with various treatments and therapies. It can also help them learn about their own personal health history and how this affects their current condition.
Overall, health education is an important tool for promoting good health throughout the population. It can helpindividuals avoid illness, learn about available resources, and make informed decisions about their care .
Methods of Teaching Health Education
One of the most important methods of teaching health education is to have students participate in hands-on activities. This allows them to learn about the body through contact and makes it easier for them to remember what they have learned. In addition, students can ask questions and get explanations from educators. Group activities also help students develop their teamwork skills.
It is also important for educators to use technology when teaching health education. This means that they can use computer-based tools, such as games, videos, and websites, to help students learn more about health topics. Additionally, educators can create their own activities using technology. This makes it fun for students and helps them stay engaged in the learning process.
Challenges in Teaching Health Education
Health education has come a long way since its inception. It is now recognized as an essential component of public health and is being offered in schools across the United States. However, despite this progress, health education faces several challenges that must be addressed if it is to be effective.
One of the main issues with health education is that it can be difficult to keep students interested in the subject matter. Many students find health-related topics tedious and abstract, making it difficult for them to retain information. This problem can be exacerbated by the fact that many health curriculums are based on outdated beliefs about disease and illness. In order to make health education more engaging for students, it is important to create materials that are based on current scientific knowledge.
Another challenge faced by health educators is the high turnover rate among students who are taught about health in school. This means that many teachers have little opportunity to develop personal relationships with their students and impart their knowledge in a meaningful way. To remedy this issue, schools should invest resources into training new teachers and providing them with adequate support materials.
Despite these challenges, there are many ways in which health education can be improved. By addressing the aforementioned issues, educators will be able to provide their students with accurate and up-to-date information about healthy living options.
Health education is an important part of keeping our citizens healthy and informed. By teaching people about their own health and the importance of taking preventive measures, we can help them live longer, healthier lives. Our goal should be to make sure that everyone in our community knows how to access quality health care if they need it, so that no one falls through the cracks.
Hopefully, by reading this article you have learned a little bit more about health education and why it is so important. As always, feel free to reach out if you have any questions or would like additional information on this topic.

Manisha Dubey Jha is a skilled educational content writer with 5 years of experience. Specializing in essays and paragraphs, she’s dedicated to crafting engaging and informative content that enriches learning experiences.
Related Posts
Essay on importance of yoga, essay on cow, climate change essay, essay on slaver, leave a comment cancel reply.
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.

45,000+ students realised their study abroad dream with us. Take the first step today
Meet top uk universities from the comfort of your home, here’s your new year gift, one app for all your, study abroad needs, start your journey, track your progress, grow with the community and so much more.

Verification Code
An OTP has been sent to your registered mobile no. Please verify

Thanks for your comment !
Our team will review it before it's shown to our readers.
- School Education /
Essay on Health: Long and Short Essay Samples

- Updated on
- Jan 3, 2024

Essay on Health:
Earlier, health was said to be the ability of the body to function well. However, as the time evolved, the definition of health also evolved. Health now, is the primary thing after which everything else follows. When you maintain good health, everything else falls into place.
In an era where our lives are increasingly busy and filled with demands, our health often takes a backseat. Yet, it’s a priceless asset that influences every facet of our existence. In this blog, we explore the multifaceted realm of health through both long and short essay samples. From the significance of well-being to practical tips for maintaining it, our collection delves into the critical role health plays in our lives. Join us in this journey to uncover the secrets of a healthier, happier life.
Table of Contents
- 1 How to Maintain Health?
- 2 Importance of Health
- 3 Sample Essay On Health in 150 Words
- 4 Sample Essay On Health in 300 Words
Must Read: Essay On My Hobby
How to Maintain Health?
Good health is above wealth. Listed foundational practices below promote overall health and well-being:
- Balanced Diet: Eat a variety of nutrient-rich foods, including fruits, vegetables, lean proteins, and whole grains. Do not miss out on the essential nutrients; take each of them in appropriate quantities.
- Regular Exercise: Exercise daily, it can be for a duration of 15-30 minutes. Include strength training exercises to build muscle and bone strength.
- Adequate Sleep: Prioritize 7-9 hours of quality sleep per night to support physical and mental well-being. Instead of using your phone, go to sleep at a reasonable hour.
- Stress Management: Practice stress-reduction techniques such as meditation, yoga, or mindfulness.
- Regular Check-ups: Schedule routine health check-ups and screenings to detect and address health issues early.
- Avoid Bad Habits: Do not smoke or drink as it has serious harmful consequences.
Importance of Health
Good health is vital for a fulfilling life. It empowers us to thrive physically, mentally, and emotionally, enhancing overall well-being. It is of paramount importance for various reasons:
- Quality of Life: It directly affects our daily lives, enabling us to enjoy activities, work, and relationships to the fullest.
- Productivity: Good health enhances productivity, allowing us to perform better in our personal and professional endeavours.
- Longevity: It contributes to a longer life, giving us more time to pursue our goals and spend time with loved ones.
- Financial Well-being: Staying healthy reduces medical expenses and the economic burden of illness.
- Emotional Well-being: Physical health is closely linked to mental well-being, impacting our mood, stress levels, and overall happiness.
- Preventive Care: Maintaining health through regular check-ups can detect and address potential issues before they become severe.
- Community and Societal Impact: Healthy individuals contribute to stronger communities and societies, reducing the strain on healthcare systems and promoting collective well-being.
Must Read: Essay On Human Rights
Sample Essay On Health in 150 Words
Maintaining good health is dependent on a lot of factors. Those factors range from the air you breathe to the type of people you choose to spend your time with. Health has a lot of components which carry equal importance. If even one of them is missing, a person cannot be completely healthy.Health is our most valuable asset. It encompasses physical, mental, and emotional well-being, shaping our lives profoundly. A healthy lifestyle, characterized by a balanced diet, regular exercise, and adequate sleep, is essential. It not only prevents diseases but also boosts energy and productivity.
Mental health is equally vital, requiring stress management and emotional support. Regular check-ups aid in early disease detection, increasing the chances of successful treatment. Good health influences longevity and quality of life, allowing us to pursue dreams and cherish moments with loved ones. It also eases the financial burden associated with illness. Ultimately, health is the foundation of a joyful, fulfilling existence, and its importance cannot be overstated.
Sample Essay On Health in 300 Words
Health is undeniably one of the most precious aspects of life. It encompasses not only the absence of diseases but also the presence of physical, mental, and emotional well-being. In this essay, we will explore the multifaceted importance of health in our lives.
Firstly, physical health is the cornerstone of our existence. It allows us to carry out daily activities, pursue our passions, and engage with the world. Maintaining good physical health involves a balanced diet that provides essential nutrients, regular exercise to keep our bodies fit, and sufficient rest to recuperate. A healthy lifestyle not only prevents various ailments but also increases our vitality and longevity.
There is this stigma that surrounds mental health. People should take mental illnesses seriously. In order to be completely fit, one must also be mentally fit. When people completely discredit mental illnesses, it makes a negative impact. Hence, we should treat mental health the same as physical health.
Mental health is equally crucial. It involves managing stress, maintaining emotional stability, and seeking support when needed. Neglecting mental health can lead to conditions like anxiety and depression, which can have a profound impact on the quality of life.
Moreover, health plays a pivotal role in determining our overall happiness and well-being. When we are in good health, we have the energy and enthusiasm to enjoy life to the fullest. It enhances our productivity at work or in our daily chores, leading to a sense of accomplishment.
Furthermore, health is closely linked to financial stability. Medical expenses associated with illness can be overwhelming. Maintaining good health through preventive measures and regular check-ups can save us from substantial healthcare costs.
In conclusion, health is not merely the absence of illness; it is the presence of physical, mental, and emotional well-being.
Related Reads:
Good health enables a fulfilling life, impacting longevity, happiness, and productivity.
Health encompasses physical, mental, and emotional well-being, signifying a state of overall vitality.
Health is evident in energy levels, a balanced mind, regular check-ups, and the ability to engage in daily activities with ease.
This brings us to the end of our blog on Essay on Health. Hope you find this information useful. For more information on such informative topics for your school, visit our essay writing and follow Leverage Edu.

Amisha Khushara
Hey there! I'm a content writer who turns complex ideas into clear, engaging stories. Think of me as your translator, taking expert knowledge and making it interesting and relatable for everyone.
Leave a Reply Cancel reply
Save my name, email, and website in this browser for the next time I comment.
Contact no. *

Connect With Us
45,000+ students realised their study abroad dream with us. take the first step today..

Resend OTP in
Need help with?
Study abroad.
UK, Canada, US & More
IELTS, GRE, GMAT & More
Scholarship, Loans & Forex
Country Preference
New Zealand
Which English test are you planning to take?
Which academic test are you planning to take.
Not Sure yet
When are you planning to take the exam?
Already booked my exam slot
Within 2 Months
Want to learn about the test
Which Degree do you wish to pursue?
When do you want to start studying abroad.
January 2025
September 2025
What is your budget to study abroad?

How would you describe this article ?
Please rate this article
We would like to hear more.
Have something on your mind?

Make your study abroad dream a reality in January 2022 with
India's Biggest Virtual University Fair

Essex Direct Admission Day
Why attend .

Don't Miss Out

Health and education
Education has the power to transform the lives of children and young people, and the world around them. At UNESCO, inclusive and transformative education starts with healthy, happy and safe learners. Because children and young people who receive a good quality education are more likely to be healthy, and likewise those who are healthy are better able to learn and complete their education.
Guided by the UNESCO Strategy on education for health and well-being , UNESCO works to improve the physical and mental health, well-being and education outcomes of all learners. By reducing health-related barriers to learning, such as gender-based violence, gender inequality, HIV and sexually transmitted infections (STIs), early and unintended pregnancy, bullying and discrimination, and malnutrition, UNESCO, governments and school systems empower learners to understand their rights, learn better and lead fulfilling lives.
What you need to know about education for health and well-being
Helping children learn about health and well-being
For healthy, informed and empowered learners
Supporting comprehensive sexuality education for adolescents and young people in Sub-Saharan Africa
Preventing and addressing violence in and around school
Key figures
is bullied at school every month globally
occur each year among adolescent girls aged 15–19
and almost half do not have handwashing facilities with water and soap
in 161 countries – nearly half of all children in primary school – receive school meals

A foundation for life and love campaign
What does comprehensive sexuality education mean to you?
A foundation for life and love
First technical brief in a series of four.

More publications

Essay on Health for Students and Children
500+ words essay on health.
Essay on Health: Health was earlier said to be the ability of the body functioning well. However, as time evolved, the definition of health also evolved. It cannot be stressed enough that health is the primary thing after which everything else follows. When you maintain good health , everything else falls into place.

Similarly, maintaining good health is dependent on a lot of factors. It ranges from the air you breathe to the type of people you choose to spend your time with. Health has a lot of components that carry equal importance. If even one of them is missing, a person cannot be completely healthy.
Constituents of Good Health
First, we have our physical health. This means being fit physically and in the absence of any kind of disease or illness . When you have good physical health, you will have a longer life span. One may maintain their physical health by having a balanced diet . Do not miss out on the essential nutrients; take each of them in appropriate quantities.
Secondly, you must exercise daily. It may be for ten minutes only but never miss it. It will help your body maintain physical fitness. Moreover, do not consume junk food all the time. Do not smoke or drink as it has serious harmful consequences. Lastly, try to take adequate sleep regularly instead of using your phone.
Next, we talk about our mental health . Mental health refers to the psychological and emotional well-being of a person. The mental health of a person impacts their feelings and way of handling situations. We must maintain our mental health by being positive and meditating.
Subsequently, social health and cognitive health are equally important for the overall well-being of a person. A person can maintain their social health when they effectively communicate well with others. Moreover, when a person us friendly and attends social gatherings, he will definitely have good social health. Similarly, our cognitive health refers to performing mental processes effectively. To do that well, one must always eat healthily and play brain games like Chess, puzzles and more to sharpen the brain.
Get the huge list of more than 500 Essay Topics and Ideas
Physical Health Alone is Not Everything
There is this stigma that surrounds mental health. People do not take mental illnesses seriously. To be completely fit, one must also be mentally fit. When people completely discredit mental illnesses, it creates a negative impact.
For instance, you never tell a person with cancer to get over it and that it’s all in their head in comparison to someone dealing with depression . Similarly, we should treat mental health the same as physical health.
Parents always take care of their children’s physical needs. They feed them with nutritious foods and always dress up their wounds immediately. However, they fail to notice the deteriorating mental health of their child. Mostly so, because they do not give it that much importance. It is due to a lack of awareness amongst people. Even amongst adults, you never know what a person is going through mentally.
Thus, we need to be able to recognize the signs of mental illnesses . A laughing person does not equal a happy person. We must not consider mental illnesses as a taboo and give it the attention it deserves to save people’s lives.
Customize your course in 30 seconds
Which class are you in.

- Travelling Essay
- Picnic Essay
- Our Country Essay
- My Parents Essay
- Essay on Favourite Personality
- Essay on Memorable Day of My Life
- Essay on Knowledge is Power
- Essay on Gurpurab
- Essay on My Favourite Season
- Essay on Types of Sports
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Download the App

- MEMBER DIRECTORY
- Member Login
- Publications
- Clinician Well-Being
- Culture of Health and Health Equity
- Fellowships and Leadership Programs
- Future of Nursing
- U.S. Health Policy and System Improvement
- Healthy Longevity
- Human Gene Editing
- U.S. Opioid Epidemic
- Staff Directory
- Opportunities
- Action Collaborative on Decarbonizing the U.S. Health Sector
- Climate Communities Network
- Communicating About Climate Change & Health
- Research and Innovation
- Culture of Health
- Fellowships
- Emerging Leaders in Health & Medicine
- Culture & Inclusiveness
- Digital Health
- Evidence Mobilization
- Value Incentives & Systems
- Substance Use & Opioid Crises
- Reproductive Health, Equity, & Society
- Credible Sources of Health Information
- Emerging Science, Technology, & Innovation
- Pandemic & Seasonal Influenza Vaccine Preparedness and Response
- Preventing Firearm-Related Injuries and Deaths
- Vital Directions for Health & Health Care
- NAM Perspectives
- All Publications
- Upcoming Events
- Past Events
- MEMBER HOME
Understanding the Relationship Between Education and Health
It is now widely recognized that health outcomes are deeply influenced by a variety of social factors outside of health care. The dramatic differences in morbidity, mortality, and risk factors that researchers have documented within and between countries are patterned after classic social determinants of health, such as education and income (Link and Phelan, 1995; CSDH, 2008), as well as placed-based characteristics of the physical and social environment in which people live—and the macrostructural policies that shape them.
A 2013 report from the National Research Council and the Institute of Medicine cited these socioecological factors, along with unhealthy behaviors and deficiencies in the health care system, as leading explanations for the “health disadvantage” of the United States. In a comparison of 17 high-income countries, age-adjusted all-cause mortality rates for 2008 ranged from 378.0 per 100,000 in Australia to 504.9 in the United States. The report found a pervasive pattern of health disadvantages across diverse categories of illness and injury that existed across age groups, sexes, racial and ethnic groups, and social classes (NRC and IOM, 2013).
Recent attention has focused on the substantial health disparities that exist within the United States, where life expectancy varies at the state level by 7.0 years for males and 6.7 years for females (NRC and IOM, 2013) but mortality and life expectancy vary even more substantially across smaller geographic areas such as counties (University of Wisconsin Population Health Institute, 2013; Kulkarni et al., 2011) and census tracts. In many U.S. cities, life expectancy can vary by as much as 25 years across neighborhoods (Evans et al., 2012). The same dramatic geographic disparities can be seen for other outcomes, such as infant mortality, obesity, and the prevalence of diabetes and other chronic diseases.
Of the various social determinants of health that explain health disparities by geography or demographic characteristics (e.g., age, gender, race-ethnicity), the literature has always pointed prominently to education. Research-based on decades of experience in the developing world has identified educational status (especially of the mother) as a major predictor of health outcomes, and economic trends in the industrialized world have intensified the relationship between education and health. In the United States, the gradient in health outcomes by educational attainment has steepened over the last four decades (Goldman and Smith, 2011; Olshansky et al., 2012) in all regions of the United States (Montez and Berkman, 2014), producing a larger gap in health status between Americans with high and low education. Among white Americans without a high school diploma, especially women, life expectancy has decreased since the 1990s, whereas it has increased for others (Olshansky et al., 2012). Death rates are declining among the most educated Americans, accompanied by steady or increasing death rates among the least educated (Jemal et al., 2008).
What accounts for the growing health advantages that exist among people with higher educational attainment? Is it what they learn in school, such as how to live a healthy lifestyle, or the socioeconomic advantages that come from an education? Or is the cross-sectional association between education and health more complex, involving numerous contextual covariables that provide a fuller back story? Despite decades of research documenting the connections between education and health, there is still much to learn about the mechanisms that enable this connection.
Unpacking the reasons for the connections between education and health is not just an exercise in scientific inquiry; it is also essential to setting policy priorities. As increasing attention is focused on the need to address social inequity in order to address health inequities, understanding the links between broad upstream factors such as education and health outcomes becomes a critical challenge. Awareness of the importance of education might help drive investment in education and improvements in educational policy.
Conceptual Framework
An overarching theoretical framework for the impact of social determinants on health is provided by an ecological model in which individuals and their behaviors are embedded, across the lifespan, within a framework of nested institutional contexts (IOM, 2000; see Figure 1). The individual and his or her characteristics are situated within and affected by the family and household, the community and its institutions (e.g., school, workplace, and civil institutions), and policies of the larger society. Each level brings access to opportunities, as well as constraints on actions and opportunities. Furthermore, these levels interact with one another, such that family resources, for example, may mediate or moderate the resources available within the community. Social scientists widely agree that unequal social status creates unequal access to resources and rewards. Social structure, as embodied in social position, structures individual behaviors and values and therefore affects many of the mediators in the relationship between education and health.
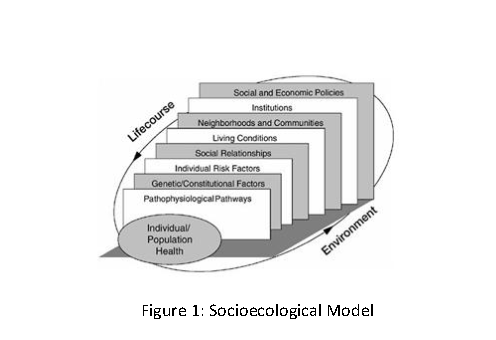
Education is one of the key filtering mechanisms that situate individuals within particular ecological contexts. Education is a driving force at each ecological level, from our choice of partner to our social position in the status hierarchy. The ecological model can therefore provide a context for the numerous ways in which education is linked to our life experiences, including health outcomes. It also provides a framework for understanding the ways in which educational outcomes themselves are conditioned on the many social and environmental contexts in which we live and how these, in turn, interact with our individual endowments and experiences.
Within this rich contextual framework, educational attainment (the number of years of schooling completed) is important but is far from the whole story. Educational attainment is often a key indicator in research studies, not least because it is often measured and recorded; life expectancy is compared by educational attainment because it is the only information about education recorded on death certificates. Besides such obvious measures of the quality of education as proficiency scores and understanding of mathematics, reading, science, and other core content, other dimensions of education are clearly important in the ecological context as well; cognitive development, character development, knowledge, critical thinking and problem solving are a few examples.
In addition, the relationship between years of education and health is not a purely linear function. As part of the literature attempting to clarify the functional form of the relationship between education and health, Montez et al. (2012) have documented a negative relationship between years of education and mortality risk for attainment less than high school graduation, a steep decline for high school graduates (with reduction of risk five times greater than attributable to other years of education), and a continued yet steeper negative relationship for additional years of schooling. The drop at high school graduation points to the importance of obtaining credentials in addition to the other benefits associated with educational attainment.
In this paper we review the health benefits associated with education, focusing on the primary mechanisms, both distal and proximate, by which education may be considered a driving force in health outcomes. We take a socioecological approach by presenting these concepts in a hierarchy, moving from the level of the person to the community/institution and then the larger social/policy context. Next, we turn to issues of causality that can make it difficult to draw conclusions about the relationship between education and health. These include reverse causality and selection , in which education may be impacted by ill health, and confounding , where both education and health are affected by some other causal factor(s) that may also provide important clues about the root causes of poor education and poor health.
The Health Benefits Associated with Education
Among the most obvious explanations for the association between education and health is that education itself produces benefits that later predispose the recipient to better health outcomes. We may think of these returns from education, such as higher earnings, as subsequent “downstream” benefits of education. Following the socioecological framework presented in the introduction, we describe a range of potential downstream impacts of education on health, starting with the ways individuals experience health benefits from education then going on to discuss the health-related community (or place-based) characteristics that often surround people with high or low education, and closing with the larger role of social context and social policy.
Impact at the Individual Level
Education can impart a variety of benefits that improve the health trajectory of the recipient. We discuss its role in enhancing noncognitive and cognitive skills and access to economic resources, and we highlight the impacts of these on health behaviors and health care usage. Although this section focuses specifically on the health benefits of education, we do so in full knowledge that education is also impacted by health, development, and a host of personal, community, and contextual factors.
Education Impacts a Range of Skills
Education contributes to human capital by developing a range of skills and traits, such as cognitive skills, problem-solving ability, learned effectiveness, and personal control (Mirowski and Ross, 2005). These various forms of human capital may all mediate the relationship between education and health.
Personality traits (also known as “soft” or noncognitive skills) are associated with success in later life, including employment and health. The “Big Five” personality factors include conscientiousness, openness to experience, extraversion, agreeableness, and neuroticism/emotional stability (Heckman and Kautz, 2012). Roberts et al. (2007) postulate three pathways whereby personality traits may impact mortality: through disease processes (e.g., response to stress), health-related behaviors, and reactions to illness. A review by Roberts et al. (2007) suggests that the strength of association between the “Big Five” personality traits and mortality is to that of IQ and stronger than socioeconomic status (SES). Although enduring, these skills are also mutable, and research indicates that educational interventions to strengthen these skills can be important, especially among children in disadvantaged areas, who may find it more difficult to refine these skills at home and in their social environments.
Personal control, also described in the literature in terms of locus of control, personal efficacy, personal autonomy, self-directedness, mastery, and instrumentalism (Ross and Wu, 1995), is another soft skill associated with educational attainment. According to the authors, “Because education develops one’s ability to gather and interpret information and to solve problems on many levels, it increases one’s potential to control events and outcomes in life. Moreover, through education one encounters and solves problems that are progressively more difficult, complex, and subtle, which builds problem-solving skills and confidence in the ability to solve problems” (Ross and Wu, 1995, p. 723).
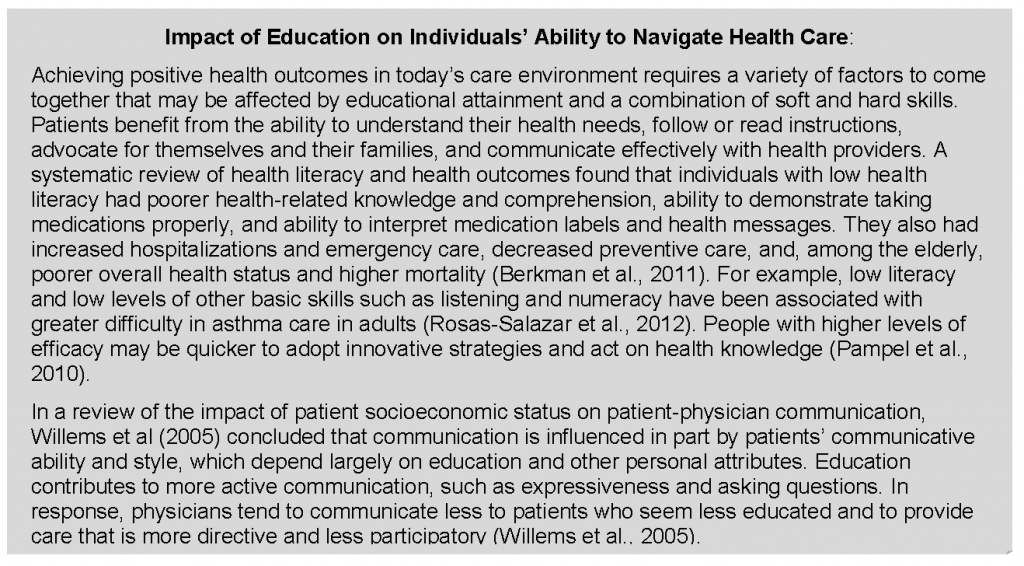
Personal control can impact individuals’ attitudes and behaviors, potentially including health behaviors. Furthermore, an individual’s sense of mastery and control may mediate stress, possibly by facilitating better coping mechanisms. Lack of personal control, on the other hand, may provoke physiological responses, leading to suppression of the immune system (Ross and Wu, 1995, p. 723).
In addition to its impact on soft skills, education has the potential to impart skills in reading, mathematics, and science/health literacy that could contribute to an individual’s health. Learners of English as a second language are helped to overcome language barriers that can interfere with understanding of health needs. Education may also improve a range of other skills, such as cognitive ability, literacy, reaction time, and problem-solving. Pathways from these skills to health outcomes may be indirect, via attainment of better socioeconomic circumstances or behavior, but they may also apply directly in understanding the increasingly complex choices individuals face in understanding health priorities and medical care needs. Skills such as higher cognitive ability and health literacy may also lead directly to improved health outcomes because of an enhanced “ability to comprehend and execute complex treatment regimens” and better disease self-management (Maitra, 2010). A strong education may be important in both navigating health care and making choices about lifestyle and personal health behaviors. Cutler and Lleras-Muney (2010) report that increased cognitive ability resulting from education contributes significantly to the education gradient in health behaviors.
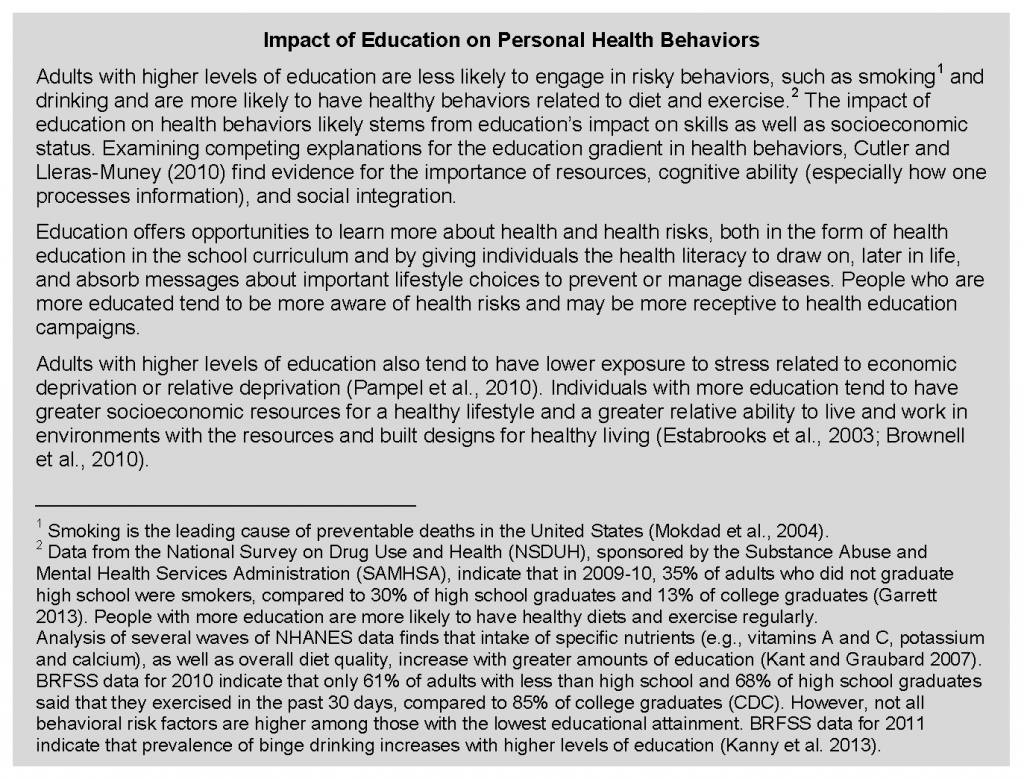
Education Increases Economic and Social Resources
A large part of the impact of education on health flows through the attainment of economic resources, such as earnings and wealth, as well social resources such as access to social networks and support. Adults with more education are less likely to experience unemployment and economic hardship and will have greater access to a variety of important material, financial and social resources. Link and Phelan (1995) point out that the specific mechanisms linking SES to health have changed over time but that SES remains a fundamental social cause of disease because it involves “access to resources that can be used to avoid risks or to minimize the consequences of disease once it occurs” (p. 87).
Economic Resources
Adults with a higher education—especially in today’s knowledge economy—have conspicuous advantages in gaining employment and finding desirable jobs (see Figure 2). Advanced degrees give workers an advantage in obtaining rewarding jobs that offer not only higher salaries and job satisfaction but other health-related benefits, such as health insurance coverage, (Adults with health insurance in the United States use more physician services and have better health outcomes compared to uninsured or inconsistently insured adults [NRC, 2009; Freeman et al., 2008; Hadley, 2003]) worksite health promotion programs, and worksite policies that protect occupational safety. An inadequate education markedly increases the risk of unemployment. (In 2012, unemployment was 12.4 percent among adults who did not graduate high school, compared to 8.3 percent among adults with a high school diploma and 4.5 percent among college graduates [BLS, 2013]. 5 A body of evidence links unemployment to adverse health outcomes. For example, a higher percentage of employed persons reported in 2010 that they were in excellent or very good health [62.7 percent] than did persons who were unemployed for less than 1 year [49.2 percent] or unemployed for more than 1 year (39.7 percent). The unemployed also reported more physically and mentally unhealthy days in the past 30 days [Athar et al., 2013]).
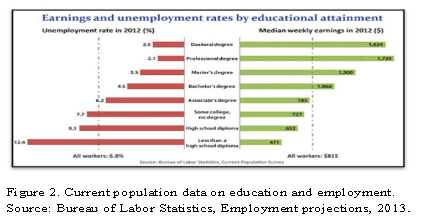
Income and wealth are leading predictors of health status (CSDH, 2008; Braveman et al., 2010), and accumulated financial strain has been shown to impact health above and beyond the effects of income and wealth (Shippee et al., 2012). In today’s society, economic resources are inextricably linked to education. In 2012, the median wage for college graduates was more than twice that of high school dropouts and more than one and a half times higher than high school graduates (BLS, 2013). Weekly earnings rise dramatically for Americans with a college or advanced degree. A higher education has an even greater effect on lifetime earnings, a pattern that is true for men and women, for blacks and whites, and for Hispanics and non-Hispanics. (According to 2006–2008 data, the lifetime earnings of a Hispanic male are $870,275 for those with less than a ninth-grade education but $2,777,200 for those with a doctoral degree. The corresponding lifetime earnings for a non-Hispanic white male are $1,056,523 and $3,403,123 [Julian and Kominski, 2011]). Economic vulnerability can affect health through a cascade effect on the ability to acquire resources that are important to health: food, stable housing, transportation, insurance, and health care (Braveman, et al., 2011). People with low income are more likely to be uninsured and to be vulnerable to the rising costs of health care, which insurance carriers are increasingly shifting to patients through higher copayments, deductibles, and premiums (In 2012, one-fourth [24.9 percent] of people in households with annual income less than $25,000 had no health insurance coverage, compared to 21.4 percent of people in households with income ranging from $25,000 to $49,999; the figure was 15.0 percent in households with income ranging from $50,000 to $74,999 and 7.9 percent with income of $75,000 or more [DeNavas-Walt et al., 2013]). Individuals with higher incomes have more resources to purchase healthy foods, to afford the time and expenses associated with regular physical activity, to have easy transportation to health care facilities or work locations, and to afford health care expenses. (According to 2010 Behavioral Risk Factor Surveillance System [BRFSS] data, 27 percent of adults with less than a high school education reported not being able to see a physician because of cost, compared to 18 percent and 8 percent of high school and college graduates, respectively [CDC, 2014]). Accordingly, the costs of a healthy lifestyle pose more of a barrier for people with less education. The health implications of these financial barriers to health care are well documented: the uninsured are less likely to receive preventive care or help with disease management (HHS, 2013, p. 9-1), and they have a higher risk of death (IOM, 2003a).
Social Resources
Educational attainment is associated with greater social support, including social networks that provide financial, psychological, and emotional support. Social support includes networks of communication and reciprocity. Individuals in a social network can relay information, define norms for behavior, and act as modeling agents. Those individuals with higher levels of education may also have higher levels of involvement with civic groups and organizations. Conversely, low social support (i.e., not participating in organizations, having few friends, being unmarried, or having lower-quality relationships) is associated with higher mortality rates (Kaplan et al., 1994; Seeman, 1996) and poor mental health (Seeman, 1996). Berkman et al. (2000) linked social integration to health outcomes in a causal chain that begins with the macrosocial and ends with psychobiological processes. They propose several mechanisms through which social integration affects health: social support, social influence, social engagement/attachment, and access to goods and resources (Berkman et al., 2000, p. 846). Social connection can be an important buffer to the negative health consequences of health stressors. Marriage imparts benefits in longevity, but weaker network ties can also have important health effects, such as the effects of peers on behavior (Smith and Christakis, 2008). The effect of social networks on smoking cessation is a well-known example (Christakis and Fowler, 2008).
Impact at the Community Level
Individuals with more education benefit not only from the resources that schooling brings to them and their families but also from health-related characteristics of the environments in which they tend to live, work, and study. Although there are many methodological challenges in estimating community-level effects on individuals (Kawachi and Berkman, 2003; Kawachi and Subramanian, 2007), communities may confer a range of benefits or risks that can impact health. In the midst of growing recognition that “place matters” to health, many studies have tried to estimate neighborhood effects on outcomes such as child/youth educational attainment, behavioral/well-being outcomes, or health status and mortality. (For example, Ross and Mirowsky (2008), using multilevel analysis of survey data from Illinois, addressed the question of whether community SES impacts health above and beyond the contributions of individual SES measures. They found that individual-level indicators of SES explained most of the variation in physical functioning (about 60 percent) but that neighborhood-level measures had a significant influence as well.) Given the wide range of methodologies and data sources utilized, findings are not uniform among such studies, but there is general agreement that a relatively modest neighborhood effect exists independent of individual and family-level factors (Kawachi and Berkman, 2003; Leventhal and Brooks-Gunn, 2000; Steptoe and Feldman, 2001). (Kawachi and Berkman (2003) call attention to the methodological difficulties of estimating neighborhood effects while controlling for individual SES, when some neighborhood effects may operate via their impact on individual outcomes, thus “adjusting away the variation of interest” (p. 9). Winkleby et al. (2006) examined the interaction between neighborhood SES and individual SES and found that low SES individuals living in higher SES neighborhoods had higher mortality rates compared to low SES individuals living in low or moderate SES neighborhoods.)) Effects that appear to occur at the neighborhood level may represent aggregated individual characteristics (compositional effects), neighborhood variability (contextual effects), or local manifestations of larger-scale processes (e.g., higher-level planning or regulatory decisions) (Shankardass and Dunn, 2011). Furthermore, it is important to recognize the dynamic interaction that occurs between the individual and the environment (Rhodes et al., 2011) and conceptions of space as “relational geographies” (Conceptualization of space as a “relational geography” emphasizes aspects such as networks rather than boundaries, social rather than physical distance, mobility of populations, and dynamic characteristics of places (Cummins et al., 2007)) (Cummins et al., 2007).
At one level, community characteristics matter because access to resources that are important to health is contingent on community-level resources and institutions. Macintyre and Ellaway (2003) categorize these as physical features, services, sociocultural features, reputation, and availability of healthy environments at home, work, and play. Theories about the mechanisms by which social environments affect the health of individuals also focus on community characteristics such as social disorganization, social control, social capital, and collective efficacy (Sampson, 2003). Kawachi et al. (2013) note that communities with higher social capital tend to be more resilient in the face of disasters and are better able to employ informal control mechanisms to prevent crime.
Through a combination of resources and characteristics, communities expose individuals to varying levels of risk versus safety (e.g., crime, unemployment, poverty, and exposure to physical hazards) and provide different levels of resources (e.g., food supply, green space, economic resources, and health care). One notable resource that differs among communities is the quality of education available. Low-income neighborhoods often have fewer good schools, not least because public schools tend to be poorly resourced by low property taxes and cannot offer attractive teacher salaries or properly maintain buildings, supplies, and school safety. Adverse community factors can compound the difficulty that children face in obtaining a good education while also compromising their health trajectory.
Below we touch on several additional community characteristics that have been linked to health outcomes, including food access, spaces and facilities for physical activity, access to health care, community economic resources, crime and violence, and environmental exposure to toxins.
- Food access. Unhealthy eating habits are linked to numerous acute and chronic health problems, such as diabetes, hypertension, obesity, heart disease, and stroke as well as higher mortality rates, but access to healthier foods tends to be limited in neighborhoods with lower median incomes and lower levels of educational attainment. In one study, access (Defined as at least one healthier food retailer within the census tract or within one-half mile of tract boundaries) to healthier food outlets was 1.4 times less likely in census tracts with fewer college-educated adults (less than 27 percent of the population) than in tracts with a higher proportion of college-educated persons; these differences varied by region and were highest in the South and lowest in the West and Northeast (Grimmet al., 2013). Conversely, low-income neighborhoods often have an oversupply of fast-food restaurants, convenience stores, bodegas, liquor stores, and other outlets that sell little fresh produce but promote inexpensive calorie-dense foods and beverages.
- Spaces and facilities for physical activity. People with higher education and income are more likely to live in neighborhoods that provide green space (e.g., parks), sidewalks, and other places that enable residents to walk and cycle to work and shopping, exercise, and outside play. Lower-income neighborhoods and those with higher proportions of nonwhite residents are also less likely to have commercial exercise facilities (Powell et al., 2006). The health benefits of green space have been documented in urban environments, especially for lower-income, young, and elderly populations (Maas et al., 2006). A longitudinal study in Great Britain found immediate, positive mental health effects of moving to urban areas with more green space (Alcock et al., 2014).
- Access to health care. Because of the maldistribution of health care providers in the United States (HHS, 1998), access to clinicians and facilities tends to be in shortest supply in rural and low-income areas. Thus, apart from whether residents have the health insurance coverage and resources to afford health care, they may struggle to find local primary care providers, specialists, and hospitals that provide quality health care services.
- Community economic resources. The lack of jobs in low-income communities can exacerbate the economic hardship that is common for people with less education, who are more likely to live in communities with a weak economic base that is unattractive to businesses, employers, and investors and are thereby often caught in a self-perpetuating cycle of economic decline and marginalization.
- Crime and violence. Community crime rates can impact health through the direct effects of violent crimes on victims, such as trauma and high youth mortality rates. Crime can also affect health indirectly, such as through fear of crime (Stafford et al., 2007) or the cumulative stress of living in unsafe neighborhoods. The high incarceration rates of residents in some communities can have deleterious effects on social networks, social capital, and social control, further compromising public health and safety (Clear, 2007). The 2006 and 2007 rounds of the American Community Survey found that, among young male high school drop-outs, nearly 1 in 10 was institutionalized on a given day in 2006–2007 versus fewer than 1 of 33 high school graduates (Sum et al., 2009).
- Environmental exposure to toxins. People of color and those with less education are more likely to live in neighborhoods that are near highways, factories, bus depots, power plants, and other sources of air and water pollution. A large body of research on environmental justice has documented the disparate exposure of low-income and minority neighborhoods to hazardous waste, pesticides, and industrial chemicals (Bullard et al., 2011; Calnan and Johnson, 1985). This exposure to toxins is perhaps the most undiscriminating place-based characteristic because residents’ personal socioeconomic advantages (e.g., education, income) offer no protection against the adverse health consequences of inhalation or ingestion of such toxins.
The Larger Social Context and Social Policy
Health inequities are driven, in large part, by the social context in which people are born, live, and work, that is, the social policies that shape resources, institutions, and laws; the economic system through which material and financial resources are created and distributed; and the social norms that govern interactions. The conditions in which people live—for example, the built environment, public transportation, urban design, crime rates, food deserts, and the location of polluting factories—are determined by macrostructural policies and the cultural values that shape them. Formulation of effective analyses and solutions to problems affecting health must address factors that go beyond the level of the individual and proximal risk factors (O’Campo and Dunn, 2011). These influences have been recognized by organizations concerned with health outcomes locally, nationally, and internationally. The World Health Organization calls for improved living and working conditions, social protection policy supportive of all, reduced inequality, and strengthened governance and civil society (CSDH, 2008). Healthy People 2020 has many policy objectives for health, including improved environmental conditions (e.g., air/water quality and exposure to hazards), violence prevention, poverty reduction, and increased rates of postsecondary education. (See http://www.healthypeople.gov/2020/topicsobjectives2020/default.aspx.) The Place Matters team in Alameda County, California, has identified five policy areas to impact health outcomes locally: economics, education, criminal justice, housing, and land use and transportation (Alameda County Public Health Department, n.d.).
Decisions made by society, voters, and policy makers—both within and outside of government—exert deep influences on education itself, as well as on the institutions and resources that populate the socioecological framework linking education and health. For example, in other societies, the adverse health consequences of poverty are often buffered by social services that act to safeguard the health of children, young parents, and other vulnerable groups. Bradley et al. (2011) found that while most OECD (Organisation for Economic Co-operation and Development) countries spent more on social services than on health expenditures, the converse was true in the United States. (The average ratio of social to health expenditures in OECD countries from 1995 to 2005 was 2.0; the ratio in the U.S. was 0.91. [Bradley et al. 2011]). Likewise, economic policies have a large influence on the employment and wealth-building opportunities of workers. Major economic and technological shifts of the last few decades have favored “nontradable” service jobs in sectors such as government and health care while manufacturing jobs have moved to less developed countries in large numbers. Remaining jobs in the “tradable” sectors such as technology and finance increasingly require advanced skill sets (Spence and Hlatshwayo, 2011). These employment trends provide a critical context in the relationship between education and health—those unable to acquire the necessary education to be competitive in an increasingly restrictive job environment are vulnerable to long-term economic hardship. Educational opportunities, however, are not equally distributed in the United States. Public school funding, largely dependent on local property taxes, varies widely both within and between states. The best-funded school systems in the United States have per pupil expenditures almost four times the per pupil expenditures in the lowest spending schools. (In 2011, total state per pupil education expenditures ranged from $6,200 to $16,700; among the 100 largest school systems in the United States, per pupil funding ranges from $5,400 to almost $20,000 [Census Bureau, 2013]). Although early studies failed to find a strong relationship between school funding amounts and student achievement, more recent meta-analysis has confirmed the importance of school funding for individual achievement (Greenwald et al., 1996).
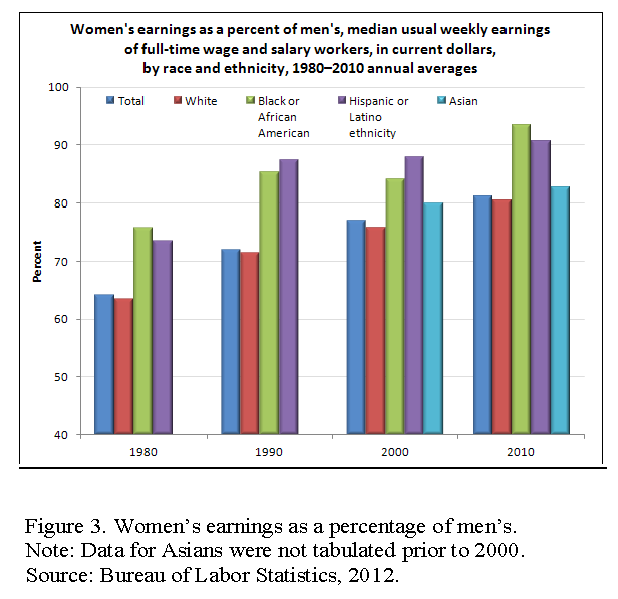
Inequality by gender, race, ethnicity, sexual orientation, and disability affect risks and opportunities for people throughout the world. Figure 3 (See Women’s earnings as percent of men’s in 2010. http://www.bls.gov/opub/ted/2012/ted_20120110.htm) shows persistent gender and race disparities in earnings. Ridgeway (2014) calls attention to the cultural as well as the material dimensions of inequality: “Cultural status beliefs work their effects on inequality primarily at the social-relational level by shaping people’s expectations for themselves and others and their consequent actions in social contexts” (p. 3). Social status hierarchies based on “categories” of difference solidify and perpetuate differentials in power and control of resources—thus leading to material inequalities. Indeed, income inequalities in the United States are significant and have become more pronounced, with wages at the lower or middle of the income distribution stagnating or falling while those at the top continue to rise. This division has continued during recovery from the Great Recession, during the first three years of which 95 percent of income gains accrued to the top 1 percent of earners (Saez, 2013). The Census Bureau reports that the Gini coefficient, which measures income inequality, has risen from 0.394 in 1970 to 0.469 in 2010; the share of household income earned by the bottom quintile was 3.3 percent in 2010, compared to 50.2 percent among the top quintile. (Table A-3: Selected Measures of Household Income Dispersion: 1967 to 2010. https://www.census.gov/hhes/www/income/data/historical/inequality/IE-1.pdf)
Historical, economic, and cultural factors play a central role in opportunities, values, and behaviors. The continuing racial residential segregation and increasing economic segregation of urban landscapes affect the life chances of those living in concentrated poverty “irrespective of personal traits, individual motivations, or private achievements” (Massey and Denton, 1993, p.3). Massey and Denton argue that residential segregation and “hypersegregation” expose residents to higher levels of social problems. Wilson (1987) links historical and economic factors in his description of the racial division of labor resulting from “decades, even centuries, of discrimination and prejudice” with the result that “because those in the low-wage sector of the economy are more adversely affected by impersonal economic shifts in advanced industrial society, the racial division of labor is reinforced” (p. 12).
Reverse Causality and Selection
Education’s association with health may reflect not only the health benefits of education but also a selection phenomenon caused by the detrimental effects of illness on educational success. Basch (2011) identifies five causal pathways by which health may impact motivation and ability to learn— sensory perceptions, cognition, school connectedness and engagement, absenteeism, and temporary or permanent dropping out (p. 596). For example, chronic health conditions can impact children’s development and educational performance (Taras and Potts-Datema, 2005). Such children are more likely to have absences for medical reasons and to be distracted by health concerns. Nonetheless, research evidence demonstrating that poor health has a causal relationship with educational outcomes is incomplete (Currie, 2009), and findings of the overall effects range from about 1.4 years reduced attainment (Estimated for 16-year-old white males from 1979 youth cohort of the National Longitudinal Surveys of Youth (NLSY) using a dynamic programming model of joint decisions of young men on schooling, work, health expenditure, and savings (Gan and Gong, 2007)) (Gan and Gong 2007) to about half a year (Goldman and Smith 2011), but there are notable exceptions. For example, evidence across countries and time periods demonstrate the harmful effect of low birth weight on education (Currie, 2009; Eide and Showalter, 2011). Disease, malnutrition, and prenatal and childhood exposures to toxins can also impact physical and cognitive development and educational achievement (Pridmore, 2007).
The extent to which reverse causality contributes to the association between education and health requires further study, but longitudinal data—the most compelling evidence to resolve the controversy—tend to suggest that most of the association is attributable to the downstream benefits of education. Eide and Showalter (2011) reviewed studies incorporating a range of methodologies that attempted to examine causal links between education and health outcomes. Studies of natural experiments in the United States (e.g., changes in compulsory school laws) generally found evidence for a causal link with mortality. Twin studies found evidence for causal links between years of schooling and self-reported health, the probability of being overweight (among men but not women), and the effects on college attendance on preventive health care later in life. Link and Phelan (1995) also discussed research attempting to show the direction of causality using quasi-experimental approaches, longitudinal designs, and analyses of risk factors that cannot be attributed to individual illness (e.g., plant closings). They concluded that these studies “demonstrated a substantial causal role for social conditions as causes of illness” (p. 83).
Conditions Throughout the Life Course That Affect Both Health and Education
A third way that education can be linked to health is when education acts as a proxy for factors throughout the life course—most notably in early childhood—that affect both education and health. For example, as noted earlier, the social and economic environment facing individuals and households and the stresses and allostatic load induced by material deprivation can affect success in school (and work) while also inducing biological changes and unhealthy behaviors that can increase the risk of disease. Although this can occur throughout the life course, increasing attention is being placed on the role of these factors on children before they reach school age.
Early Childhood Experiences
The education community has long understood the connections between early life experiences and educational success. It is well established that school readiness is enhanced by positive early childhood conditions—for example, fetal well-being and social-emotional development (Denhem, 2006), family socioeconomic status, (Children’s birth weight, developmental outcomes, health status (e.g., obesity and specific health conditions), disability, and success in school are strongly linked to parents’ education and family income and assets (Williams Shanks and Robinson, 2013; Chapman et al., 2008; Currie, 2009)) neighborhood socioeconomic status (Jencks and Mayer, 1990; Mayer and Jencks, 1989), and early childhood education (Barnett and Belfield, 2006) — but some of these same exposures also appear to be vital to the health and development of children and their future risk of adopting unhealthy behaviors and initiating adult disease processes.
Below are several examples from the literature of early childhood experiences that influence health.
- Low birth weight affects not only educational outcomes but also health and disability (Avchen et al., 2001).
- Nurturing relationships beginning at birth, the quality of the home environment, and access to stimulation provide a necessary foundation for children to grow and thrive (Heckman, 2006). One example of this is the importance of child-directed speech during infancy for language skills (Weisleder and Fernald, 2013). The effects of stress can be reduced when children have a responsive and supportive caregiver available to help cope with stress and provide a protective effect (Shonkoff and Garner, 2012).
- Unstable home and community life, such as economic factors, family transitions, housing instability, and school settings, can harm child development and later outcomes (Sandstromand Huerta, 2013). In one study, (Data were based on research by the National Poverty Center on the basis of the Michigan Recession and Recovery Study (MRRS) of adults ages 19–64 in southeastern Michigan. The researchers examined the relationship between various forms of housing instability and health, controlling for prior health problems and sociodemographic characteristics) homelessness and struggles with mortgage payments and foreclosure were predictive of self-rated health, and these combined with other categories (e. g., moved for cost in past 3 years, behind on rent) also predicted mental health problems (Burgard et al., 2012).
- Family and neighborhood socioeconomic status not only affect education but also predict developmental and health trajectories as children grow and develop (Case et al., 2002; Duncan et al.,1994). Duration and timing of childhood poverty are important. Longitudinal studies indicate that the largest effects of poverty on child outcomes are during early childhood development, when children experience poverty for multiple years, and when they live in extreme poverty (Brooks-Gunn and Duncan 1997). Guo (1998) also found that timing of poverty during early adolescence is important for adolescent achievement.
Biological Pathways
A growing body of research suggests that the similar root causes that lead children to poor educational outcomes and poor health outcomes may not operate via separate pathways but may relate to the biology of brain development and the pathological effects of early childhood exposure to stress and adverse childhood events (ACEs). Children in low SES households are more likely to experience multiple stressors that can harm health and development (Evans and Kim, 2010), mediated by chronic stress (Evans et al., 2011). These disruptions, along the pathways listed below, can thereby shape educational, economic, and health outcomes decades and generations later (NRC and IOM, 2000).
- Neuroanatomy and neuroplasticity: Infants and toddlers exposed to toxic stress, social exclusion and bias, persistent poverty, and trauma may experience changes in brain architecture and development that affect cognition, the ability to learn new skills, behavioral and stress regulation, executive function, and the capacity to adapt to future adversity (Hackman, 2010; Gottesman and Hanson, 2005).
- Endocrine disruption: Early life stressors also appear to cause physiological increases in allostatic load that promote stress-related diseases later in life (Shonkoff and Garner, 2012). Such stressors may, for example, disrupt the hypothalamic-pituitary-adrenal axis of the endocrine system and stimulating overproduction of stress-related hormones that are thought to adversely affect end organs and lead later in life to heart disease and other adult health problems (McEwen, 2012).
- Immune dysregulation: The release of interleukins and other immune reactant proteins is thought to create conditions of chronic inflammation that may increase the risk of heart disease and other chronic diseases later in life (McEwen, 2012).
- Epigenetic changes: Chronic stress is thought to affect methylation of DNA and cause epigenetic changes that “turn on” expression of genes that may cause cancer and other diseases (Zhang and Meaney, 2010).
Enhanced understanding of these biological pathways is shedding light on research, first reported in the 1990s, that called attention to the correlation between adult disease rates and a history of childhood exposure to ACEs. In a seminal study on the subject, the Adverse Childhood Experiences study, Felitti et al. (1998) surveyed more than 13,000 adult patients at Kaiser Permanente and asked whether they recalled exposure to seven categories of ACEs: psychological, physical, or sexual abuse; violence against the mother; living in a household with members who are substance abusers; mentally ill or suicidal; or imprisonment (Felitti et al., 1998). More than half the adults recalled ACEs as children, and those with greater trauma were more likely to report unhealthy behaviors as adults (e.g., smoking, physical inactivity, alcoholism, drug abuse, multiple sexual partners) and to have a history of depression or a suicide attempt. The researchers reported a dose-response relationship: those who recalled four categories of ACEs faced significant odds ratios for adult diseases, including ischemic heart disease (2.2), cancer (1.9), stroke (2.4), chronic lung disease (3.9), and diabetes (1.6).
The ACE study and subsequent studies with similar results relied on retrospective designs that faced the limitation of recall bias (relying on the memory of adults); recollections of ACEs were vulnerable to the criticism that sick adults might have skewed perceptions of their childhood experiences. Nevertheless, prospective studies that documented ACEs contemporaneously during childhood have also documented higher rates of disease when the children were followed into adulthood. The Centers for Disease Control and Prevention maintains a website that is cataloguing the burgeoning research on ACEs (CDC, 2014), and increasing attention is shifting toward strategies for policy and clinical practice to help ameliorate childhood exposure to ACEs and to buffer their adverse biological and psychosocial effects.
The building evidence that stress and other contextual factors can have effects on both education and health throughout the life course—as in the lasting effects on development, behavior, learning, and health of children—adds important insights for understanding the correlation between education and health. As discussed earlier in this paper, reverse causality plays some role in the association, and a much larger influence comes from the downstream benefits of education (e.g., greater socioeconomic resources and personal skills), but the upstream influence of adverse experiences on the young child also cannot be ignored. The effects of ACEs on the developing brain and on behavior can affect performance in school and explain setbacks in education—but it can also affect health outcomes. Thus, the correlation between reduced education and illness may have as much to do with the seeds of illness that are planted before children ever reach school age than with the consequences of education itself. They end up with fewer years of education and greater illness, but an important way to improve their health is to address the root causes that expose children to stress in the first place.
- Alameda County Public Health Department. n.d. Place matters. Available at: www.acphd.org/media/114473/placematters_overview.pdf (accessed April 10, 2014).
- Alcock, I., M. P. White, B. W. Wheeler, L. E. Fleming, and M. H. Depledge. 2014, Longitudinal effects on mental health of moving to greener and less green urban areas. Environmental Science and Technology 48(2):1247–1255. https://doi.org/10.1021/es403688w
- Athar, H. M., M. H. Chang, R. A. Hahn, E. Walker, and P. Yoon. 2013. Unemployment—United States, 2006 and 2010. CDC health disparities and inequalities report—United States, Centers for Disease Control. Morbidity and Mortality Weekly Report 62(3):27–32. Available at: http://www.cdc.gov/mmwr/pdf/other/su6203.pdf (accessed February 7, 2014).
- Avchen, R. N., G. Scott, and C. A. Mason. 2001. Birth weight and school-age disabilities: A population-based study. American Journal of Epidemiology 154(10):895–901. https://doi.org/10.1093/aje/154.10.895
- Barnett, W. S., and C. R. Belfield. Early childhood development and social mobility. 2006. The Future of Children 16(2):73–98. https://doi.org/10.1353/foc.2006.0011
- Basch, C. E. 2011. Healthier students are better learners: A missing link in school reforms to close the achievement gap. Journal of School Health 81(10):593–598. Available at: https://healthyschoolscampaign.org/wp-content/uploads/2017/03/A-Missing-Link-in-School-Reforms-to-Close-the-Achievement-Gap.pdf (accessed May 26, 2020).
- Berkman, L. F., T. Glass, I. Brissette, T. E. Seeman. 2000. From social integration to health: Durkheim in the new millennium. Social Science and Medicine 51:843–857. https://doi.org/10.1016/s0277-9536(00)00065-4
- Berkman, N. D., S. L. Sheridan, K. E. Donahue, D. J. Halpern, and K. Crotty. 2011. Low health literacy and health outcomes: An updated systematic review. Annals of Internal Medicine 155(2):97–107. https://doi.org/10.7326/0003-4819-155-2-201107190-00005
- BLS (Bureau of Labor Statistics). 2013. Employment projections. Available at: http://www.bls.gov/emp/ep_chart_001.htm (accessed February 7, 2014).
- BLS. Women’s earnings as a percent of men’s in 2010. 2012. Available at: http://www.bls.gov/opub/ted/2012/ted_20120110.htm (accessed June 3, 2014).
- Boote, J., R. Telford, and C. Cooper. 2002. Consumer involvement in health research: A review and research agenda. Health Policy 61:213–236. https://doi.org/10.1016/s0168-8510(01)00214-7
- Bradley E. H., B. R. Elkins, J. Herrin, and B. Elbel. 2011. Health and social services expenditures: Associations with health outcomes. BMJ Quality and Safety 20:826–831. https://doi.org/ 10.1136/bmjqs.2010.048363.
- Braveman, P., S. Egerter, and C. Barclay. 2011. Issue Brief Series: Exploring the Social Determinants of Health: Income, Wealth, and Health. Princeton, NJ, Robert Wood Johnson Foundation. Available at: https://www.rwjf.org/en/library/research/2011/04/how-social-factors-shape-health1.html (accessed May 26, 2020).
- Braveman, P. A., C. Cubbin, S. Egerter, D. R. Williams, and E. Pamuk. 2010. Socioeconomic disparities in health in the United States: What the patterns tell us. American Journal of Public Health 100(Suppl. 1):S186–S196. https://doi.org/10.2105/AJPH.2009.166082
- Brooks-Gunn, J., and G. J. Duncan. 1997. The effects of poverty on children. The Future of Children: Children and Poverty 7:55–71. Available at: https://pubmed.ncbi.nlm.nih.gov/9299837/ (accessed May 26, 2020).
- Brotaneka, J. M., C. E. Seeley, and G. Flores. 2008. The importance of cultural competency in general pediatrics. Current Opinion in Pediatrics 20:711–718. https://doi.org/10.1097/MOP.0b013e328317efff
- Brownell, K. D., R. Kersh, D. S. Ludwig, R. C. Post, R. M. Puhl, M. B. Schwartz, and W. C. Willett. 2010. Personal responsibility and obesity: A constructive approach to a controversial issue. Health Affairs 29(3):379–387. https://doi.org/10.1377/hlthaff.2009.0739
- Bullard, R. D., G. S. Johnson, and A. O. Torres. 2011. Environmental health and racial equity in the United States: Building environmentally just, sustainable and livable communities. Washington, DC: American Public Health Association. Available at: https://hefn.org/learn/resource/environmental_health_and_racial_equity_in_the_united_states_building_environmentally (accessed May 26, 2020).
- Burgard, S., K. Seefeldt, and S. Zelner. 2012. Housing instability and health: Findings from the Michigan Recession and Recovery Study. Population Studies Center Research Report 12-749. Ann Arbor, MI: University of Michigan Institute for Social Research. Available at: http://www.psc.isr.umich.edu/pubs/pdf/rr12-749.pdf (accessed February 26, 2014).
- Calnan, M. and Johnson, B. 1985. Health, health risks, and inequalities: An exploratory study of women’s perceptions. Sociology of Health and Illness (7): 55-75. https://doi.org/10.1111/1467-9566.ep10831360
- Case, A., D. Lubotsky, and C. Paxson. 2002. Economic status and health in childhood: The origins of the gradient. American Economic Review 92:1308–1334. https://doi.org/10.1257/000282802762024520
- CDC (Centers for Disease Control). 2014. Behavioral Risk Factor Surveillance System, 2010 BRFSS data. Office of Surveillance, Epidemiology, and Laboratory Services. Available at: http://www.cdc.gov/brfss/data_tools.htm (accessed February 14, 2014).
- Chapman, D. A., K. G. Scott, and T. L. Stanton-Chapman. 2008. Public health approach to the study of mental retardation. American Journal on Mental Retardation 113(2):102–116. Available at: http://meridian.allenpress.com/ajidd/article-pdf/113/2/102/2027787/0895-8017(2008)113[102_phatts]2_0_co_2.pdf (accessed May 28, 2020).
- Christakis, N. A., and J. H. Fowler. 2008. The collective dynamics of smoking in a large social network. New England Journal of Medicine 358:2249–2258. https://doi.org/10.1056/NEJMsa0706154
- Clear, T. R. 2007. Impact of incarceration on community public safety and public health. In Public health behind bars: From prisons to communities, edited by R. B Greifinger, J. A. Bick, and J. Goldenson. New York: Springer. Pp. 13–24.
- CSDH (Commission on Social Determinants of Health). 2008. Closing the gap in a generation: Health equity through action on the social determinants of health. Geneva, Switzerland: World Health Organization, Commission on Social Determinants of Health. Available at: http://www.who.int/social_determinants/thecommission/finalreport/en/ (accessed April 11, 2014).
- Cummins, S., S. Curtis, A. V. Diez-Roux, and S. Macintyre. 2007. Understanding and representing “place” in health research: A relational approach. Social Science and Medicine 65:1825–1838. https://doi.org/ 10.1016/j.socscimed.2007.05.036
- Currie, J. 2009. Healthy, wealthy, and wise: Socioeconomic status, poor health in childhood, and human capital development. Journal of Economic Literature 47(1):87–122. https://doi.org/10.1257/jel.47.1.87
- Cutler, D. M., and A. Lleras-Muney. 2010. Understanding differences in health behaviors by education. Journal of Health Economics 29(1):1–28. https://doi.org/10.1016/j.jhealeco.2009.10.003
- DeNavas-Walt, C., B. D. Proctor, and J. C. Smith. 2013. Income, poverty, and health insurance coverage in the United States: Current population reports. U.S. Department of Commerce, Economics and Statistics Administration, U.S. Census Bureau. September. Available at: http://www.census.gov/hhes/www/hlthins/ (accessed May 23, 2014).
- Denhem, S. A. 2006. Social-emotional competence as support for school readiness: What is it and how do we assess it? Early Education and Development 17(1):57–89. https://doi.org/10.1207/s15566935eed1701_4
- Duncan, G. J., J. Brooks-Gunn, and P. K. Klebanov. 1994. Economic deprivation and early childhood development. Child Development 65:296–318. https://doi.org/10.2307/1131385
- Eide, R. E., and M. H. Showalter. 2011. Estimating the relation between health and education: What do we know and what do we need to know? Economics of Education Review 30(5):778–791. Available at: http://www.sciencedirect.com/science/article/pii/S0272775711000525 (accessed May 28, 2020).
- Estabrooks, P. A., R. E. Lee, and N. C. Gyurcsik. 2003. Resources for physical activity participation: Does availability and accessibility differ by neighborhood socioeconomic status? Annals of Behavioral Medicine 25(2):100–104. https://doi.org/10.1207/S15324796ABM2502_05
- Evans, B. F., E. Zimmerman, S. H. Woolf, and A. D. Haley. 2012. Social determinants of health and crime in post-Katrina Orleans Parish. Richmond: Virginia Commonwealth University Center on Human Needs.
- Evans, G. W., J. Brooks-Gunn, and P. K. Klebanov. 2011. Stressing out the poor: Chronic physiological stress and the income-achievement gap. Community Investments 23(2):22–27. Available at: https://inequality.stanford.edu/sites/default/files/PathwaysWinter11_Evans.pdf (accessed May 28, 2020).
- Evans, G. W., and P. Kim. 2010. Multiple risk exposure as a potential explanatory mechanism for the socioeconomic status-health gradient. Annals of the New York Academy of Sciences 186(1):174–189. https://doi.org/10.1111/j.1749-6632.2009.05336.x
- Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M.Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine 14(4):245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
- Freeman, J. D., S. Kadiyala, J. F. Bell, and D. P. Martin. 2008. The causal effect of health insurance on utilization and outcomes in adults: A systematic review of U.S. studies. Medical Care 46(10):1023–1032. https://doi.org/10.1097/MLR.0b013e318185c913
- Gan, L., and G. Gong. 2007. Estimating interdependence between health and education in a dynamic model. NBER Working Paper No. 12830, Cambridge, MA. Available at: http://www.nber.org/papers/w12830 (accessed April 2, 2014).
- Garrett, B. E., S. R. Dube, C. Winder, and R. S. Caraballo. 2013. Cigarette smoking—United States, 2006–2008 and 2009–2010. DC health disparities and inequalities report—United States, 2013. Centers for Disease Control. Morbidity and Mortality Weekly Report 62(3):81–84. Available at: http://www.cdc.gov/mmwr/pdf/other/su6203.pdf (accessed February 7, 2014).
- Gaston, G. B. 2013. African-Americans’ perceptions of health care provider cultural competence that promote HIV medical self-care and antiretroviral medication adherence. AIDS Care 25(9):1159–1165. Available at: http://www.tandfonline.com/doi/abs/10.1080/09540121.2012.752783#preview (accessed, May 23, 2014).
- Goldman, D., and J. P. Smith. 2011. The increasing value of education to health. Social Science and Medicine 72:1728–1737. https://doi.org/ 10.1016/j.socscimed.2011.02.047
- Gottesman, I. I., and D. R. Hanson. 2005. Human development: Biological and genetic processes. Annual Review of Psychology 56:263-286. https://doi.org/10.1146/annurev.psych.56.091103.070208
- Greenwald, R., L. V. Hedges, and R. D. Laine. 1996. The effect of school resources on student achievement. Review of Educational Research 66(3):361–396. https://doi.org/10.2307/1170528
- Grimm, K. A., L. V. Moore, and K. S. Scanlon. 2013. Access to health food retailers—Unites States, 2011. CDC health disparities and inequalities report—United States, 2013. Centers for Disease Control. Morbidity and Mortality Weekly Report 62(3):20–26. Available at: http://www.cdc.gov/mmwr/pdf/other/su6203.pdf (accessed February 7, 2014).
- Guo, G. 1998. The timing of influences of cumulative poverty on children’s cognitive ability and achievement. Social Forces 77(1):257–287. https://doi.org/10.2307/3006017
- Hackman, D. A., M. J. Farah, and M. J. Meaney. 2010. Socioeconomic status and the brain: Mechanistic insights from human and animal research. Nature Reviews Neuroscience 11: 651-659. https://doi.org/10.1038/nrn2897
- Hadley, J. 2003. Sicker and poorer—the consequences of being uninsured: A review of the research on the relationship between health insurance, medical care use, health, work, and income. Medical Care Research and Review 60(Suppl. 2):S3–S75. https://doi.org/10.1177/1077558703254101
- Heckman, J. J. 2006. Skill formation and the economics of investing in disadvantaged children. Science 312:1900–1902. Available at: http://jenni.uchicago.edu/papers/Heckman_Science_v312_2006.pdf (accessed May 28, 2020).
- Heckman, J. J., and T. Kautz. 2012. Hard evidence on soft skills. Labour Economics 19:451–464. https://doi.org/10.1016/j.labeco.2012.05.014
- HHS (Health and Human Services). 1998. Council on graduate medical education tenth report: Physician distribution and health care challenges in rural and inner-city areas. Public Health Service, Health Resources and Services Administration. Available at: http://www.hrsa.gov/advisorycommittees/bhpradvisory/cogme/Reports/tenthreport.pdf (accessed February 14, 2014).
- HHS. 2013. National healthcare quality report 2012. Agency for Healthcare Research and Quality, Rockville, MD. Available at: http://www.ahrq.gov/research/findings/nhqrdr/nhqr12/nhqr12_prov.pdf (accessed February 14, 2014).
- Institute of Medicine. 2000. Promoting Health: Intervention Strategies from Social and Behavioral Research . Washington, DC: The National Academies Press. https://doi.org/10.17226/9939
- Institute of Medicine. 2003. Hidden Costs, Value Lost: Uninsurance in America . Washington, DC: The National Academies Press. https://doi.org/10.17226/10719
- Institute of Medicine. 2003. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care . Washington, DC: The National Academies Press. https://doi.org/10.17226/12875
- Jemal, A., E. Ward, R. N. Anderson, T. Murray, and M. J. Thun. 2008. Widening of socioeconomic inequalities in U.S. death rates, 1993–2001. PLoS ONE 3(5):1–8. https://doi.org/10.1371/journal.pone.0002181
- National Research Council. 1990. Inner-City Poverty in the United States . Washington, DC: The National Academies Press. https://doi.org/10.17226/1539
- Julian, T. A., and R. A. Kominski. 2011. Education and synthetic work-life earnings estimates. American Community Survey Reports, ACS-14. U.S. Census Bureau, Washington, DC. Available at: https://www.census.gov/library/publications/2011/acs/acs-14.html (accessed May 28, 2020).
- Kanny, D., Y. Liu, R. D. Brewer, and H. Lu. 2013. Binge drinking–United States, 2011. CDC health disparities and inequalities report—United States, 2013. Centers for Disease Control. Morbidity and Mortality Weekly Report 62(3):77–80. Available at: http://www.cdc.gov/mmwr/pdf/other/su6203.pdf (accessed February 7, 2014).
- Kant, A. K., and B. I. Graubard. 2007. Secular trends in the association of socio-economic position with self-reported dietary attributes and biomarkers in the U.S. population: National Health and Nutrition Examination Survey (NHANES) 1971–1975 to NHANES 1999–2002. Public Health Nutrition 10(2):158–167. https://doi.org/10.1093/ajcn/84.5.1215
- Kaplan, G. A., T. W. Wilson, R. D. Cohen, J. Kauhanen, M. Wu, and J. T. Salonen. 1994. Social functioning and overall mortality: Prospective evidence from the Kuopio Ischemic Heart Disease Risk Factor Study. Epidemiology 5(5):495–500. Available at: https://pubmed.ncbi.nlm.nih.gov/7986863/ (accessed May 28, 2020).
- Karlamangla, A. S., H. S. Burton, and T. E. Seeman. 2006. Reduction in allostatic load in older adults is associated with lower all-cause mortality risk: MacArthur studies of successful aging. Psychosomatic Medicine 68:500–507. https://doi.org/10.1097/01.psy.0000221270.93985.82
- Kawachi, I., and L. F. Berkman. 2003. Neighborhoods and health. New York: Oxford University Press.
- Kawachi, I., and S. V. Subramanian. 2007. Neighbourhood influences on health. Journal of Epidemiology and Community Health 61(1):3–4. https://doi.org/10.1136/jech.2005.045203
- Kawachi, I., S. Takao, and S. V. Subramanian, eds. 2013. Global perspectives on social capital and health. New York: Springer.
- Krueger, P. M., and V. Chang. 2008. Being poor and coping with stress: Health behaviors and the risk of death. American Journal of Public Health 98:889–896. https://doi.org/10.2105/AJPH.2007.114454
- Kulkarni, S. C., A. Levin-Rector, M. Ezzati, and C. J. Murray. 2011. Falling behind: life expectancy in U.S. counties from 2000 to 2007 in an international context. Population Health Metrics 9(1):16. https://doi.org/10.1186/1478-7954-9-16
- Leventhal, T., and J. Brooks-Gunn. 2000. The neighborhood they live in: The effects of neighborhood residence on child and adolescent outcomes. Psychological Bulletin 126(2):309–337. https://doi.org/10.1037/0033-2909.126.2.309
- Link, B. G., and J. Phelan. 1995. Social conditions as fundamental causes of disease. Journal of Health and Social Behavior 36:80–94. https://doi.org/10.1177/0022146510383498
- Maas, J., R. A., Verheij, P. P. Groenewegan, S. de Vries, and P. Spreeuwenberg. 2006 Green space, urbanity, and health: How strong is the relation? Journal of Epidemiology and Community Health 60:587–592. https://doi.org/10.1136/jech.2005.043125
- Macintyre, S., and A. Ellaway A. 2003. Neighborhoods and health: An overview. In Neighborhoods and health, edited by I. Kawachi and L. F. Berkman. New York: Oxford University Press. Pp. 20–42.
- Maitra, S. 2010. Can patient self-management explain the health gradient? Goldman and Smith’s “Can patient self-management help explain the SES health gradient?” (2002) revisited. Social Science and Medicine 70:802–812. https://doi.org/10.1016/j.socscimed.2009.08.043
- Massey, D. S., and N. A. Denton. 1993. American apartheid: Segregation and the making of the underclass. Cambridge, MA: Harvard University Press.
- Mayer, S. E., and C. Jencks. 1989. Growing up in poor neighborhoods: How much does it matter? Science 243(4897):1441–1445. https://doi.org/10.1126/science.243.4897.1441
- McEwen, B.S. 2012. Brain on stress: How the social environment gets under the skin. Proceedings of the National Academy of Sciences 109(2):17180-17185. https://doi.org/ 10.1073/pnas.1121254109
- McEwen, B. S., and E. Stellar. 1993. Stress and the individual: Mechanisms leading to disease. Archives of Internal Medicine 153(18):2093–2101. Available at: https://pubmed.ncbi.nlm.nih.gov/8379800/ (accessed May 28, 2020).
- Mirowsky, J., and C. E. Ross. 2005. Education, learned effectiveness and health. London Review of Education 3(3):205–220. Available at: https://eric.ed.gov/?id=EJ821180 (accessed May 28, 2020).
- Mistry K. B., C. S. Minkovitz, A. W. Riley, S. B. Johnson, H. A. Grason, L. C. Dubay, and B. Guyer.. 2012. A new framework for childhood health promotion: the role of policies and programs in building capacity and foundations of early childhood health. American Journal of Public Health 102: 1688-1696. https://doi.org/10.2105/AJPH.2012.300687
- Mokdad, A. H., J. S. Marks, D. F. Stroup, and J. L. Gerberdin. 2004. Actual causes of death in the United States 2000. Journal of American Medical Association 291(10):1238–1245. https://doi.org/10.1001/jama.291.10.1238
- Montez, J. K., and L. F. Berkman. 2014. Trends in the educational gradient of mortality among U.S. adults aged 45 to 84 years: Bringing regional context into the explanation. American Journal of Public Health 104(1):e82–e90. https://doi.org/10.2105/AJPH.2013.301526
- Montez, J. K., R. A. Hummer, and M. D. Hayward. 2012. Educational attainment and adult mortality in the United States: A systematic assessment of functional form. Demography 45:315–336. https://doi.org/10.1007/s13524-011-0082-8
- Institute of Medicine. 2009. America’s Uninsured Crisis: Consequences for Health and Health Care . Washington, DC: The National Academies Press. https://doi.org/10.17226/12511
- Institute of Medicine and National Research Council. 2000. From Neurons to Neighborhoods: The Science of Early Childhood Development . Washington, DC: The National Academies Press. https://doi.org/10.17226/9824
- Institute of Medicine and National Research Council. 2013. U.S. Health in International Perspective: Shorter Lives, Poorer Health . Washington, DC: The National Academies Press. https://doi.org/10.17226/13497
- O’Campo, P., and J. R. Dunn, eds. 2011. Rethinking social epidemiology. Dordrecht: Springer. Available at: http://www.cdc.gov/nchs/data/databriefs/db82.pdf (accessed May 23, 2014).
- Olshansky, S. J., T. Atonucci, L. Berkman, R. H. Binstock, A. Boersch-Supan, J. T. Cacioppo, B. A. Carnes, L. L. Carstensen, L. P. Fried, D. P. Goldman, J. Jackson, M. Kohli, J. Rother, Y. Zheng, and J. Rowe. 2012. Differences in life expectancy due to race and educational differences are widening, and many may not catch up. Health Affairs 31:1803-1813. https://doi.org/ 10.1377/hlthaff.2011.0746
- Pampel, F. C., P. M. Krueger, and J. T. Denney. 2010. Socioeconomic disparities in health behaviors. Annual Review of Sociology 36:349–370. https://doi.org/10.1146/annurev.soc.012809.102529
- Pearlin, L. I. 1989. The sociological study of stress. Journal of Health and Social Behavior 30(3):241–256. https://doi.org/10.2307/2136956
- Powell, L. M., S. Slater, F. J. Chaloupka, and D. Harper. 2006. Availability of physical activity-related facilities and neighborhood demographic and socioeconomic characteristics: A national study. American Journal of Public Health 96:1676–1680. https://doi.org/10.2105/AJPH.2005.065573
- Pridmore, P. 2007. Impact of health on education access and achievement: A cross-national review of the research evidence. Create Pathways to Access Research Monograph No. 2. Consortium for Research on Educational Access, Transitions and Equity. Institute of Education, University of London. Available at: http://files.eric.ed.gov/fulltext/ED508614.pdf (accessed April 29, 2014).
- Rhodes, T., K Wagner, S. A. Strathdee, K. Shannon, P. Davidson, and P. Bourgois. 2011. Structural violence and structural vulnerability within the risk environment: Theoretical and methodological perspectives for a social epidemiology of HIV risk among injection drug users and sex workers. In Rethinking social epidemiology, edited by P. O’Campo and J. R. Dunn. Dordrecht: Springer. Pp 205–230.
- Ridgeway, C. L. 2014. Why status matters for inequality. American Sociological Review 79(1):1–16. Available at: https://www.asanet.org/sites/default/files/savvy/journals/ASR/Feb14ASRFeature.pdf (accessed May 28, 2020).
- Roberts, B. W., N. R. Kuncel, R. Shiner, A. Caspi, and L. R. Goldberg. 2007. The power of personality: The comparative validity of personality traits, socioeconomic status, and cognitive ability for predicting important life outcomes. Perspectives on Psychological Science 2(4):313–345. https://doi.org/10.1111/j.1745-6916.2007.00047.x
- Rosas-Salazar, C., A. J. Apter, G. Canino, and J. C. Celedon. 2008. Neighborhood socioeconomic status and health: Context or composition? City and Community 7(2):163–179. https://doi.org/10.1111/j.1540-6040.2008.00251.x
- Rosas-Salazar, C., A. J. Apter, G. Canino, and J. C. Celedon. 2012. Health literacy and asthma. Journal of Allergy and Clinical Immunology 129(4):935–942. https://doi.org/10.1016/j.jaci.2012.01.040
- Ross, C. E., and C. L. Wu. 1995. The links between education and health. American Sociological Review 60(5):719–745. https://doi.org/10.2307/2096319
- Saez, E. 2013. Striking it richer: The evolution of top incomes in the United States (updated with 2012 preliminary estimates). Available at: http://elsa.berkeley.edu/~saez/saez-UStopincomes-2012.pdf (accessed May 23, 2014).
- Sampson, R. J. 2003. Neighborhood-level context and health: Lessons from sociology. In Neighborhoods and health, edited by I. Kawachi and L. F. Berkman. New York: Oxford University Press. Pp. 132–146.
- Sandstrom, H., and S. Huerta. 2013. The negative effects of instability on child development: A research synthesis. Low-Income Working Families Discussion Paper 3. Washington, DC: Urban Institute. Available at: https://www.urban.org/sites/default/files/publication/32706/412899-The-Negative-Effects-of-Instability-on-Child-Development-A-Research-Synthesis.PDF (accessed May 28, 2020).
- Seeman, T. E. 1996. Social ties and health: The benefits of social integration. Annals of Epidemiology 6(5):442–451. https://doi.org/10.1016/s1047-2797(96)00095-6
- Seeman, T. E., B. H. Singer, J. W. Rowe, R. I. Horwitz, and B. S. McEwen. 1997. Price of adaptation: Allostatic load and its health consequences. Archives of Internal Medicine 157:2259–2268. Available at: https://pubmed.ncbi.nlm.nih.gov/9343003/ (accessed May 28, 2020).
- Shankardass, K., and J. R. Dunn. 2011. How goes the neighbourhood? Rethinking neighbourhoods and health research in social epidemiology. In Rethinking social epidemiology, edited by P. O’Campo and J. R. Dunn. Dordrecht: Springer. Pp 137–156.
- Shippee, T. P., L. R. Wilkinson, and K. F. Ferraro. 2012. Accumulated financial strain and women’s health over three decades. Journals of Gerontology Series B: Psychological Sciences and Social Sciences I 67(5):585–594, https://doi.org/10.1093/geronb/gbs056
- Shonkoff, J. P., and A. S. Garner. 2012. The lifelong effects of early childhood toxic stress. Pediatrics 129(1):e232–e246. https://doi.org/10.1542/peds.2011-2663
- Shonkoff J. P., W. T. Boyce, and B. S. McEwen. 2009. Neuroscience, molecular biology, and the childhood roots of health disparities: building a new framework for health promotion and disease prevention. JAMA 301(21): 2252-2259. https://doi.org/10.1001/jama.2009.754
- Smith, K. P., and N. A. Christakis. 2008. Social networks and health. Annual Review of Sociology 34:405–429. Available at: http://www.pinniped.net/smith2008.pdf (accessed May 28, 2020).
- Spence, M., and S. Hlatshwayo. 2011. The evolving structure of the American economy and the employment challenge. New York: Council on Foreign Relations. Available at: http://www.cfr.org/industrialpolicy/evolving-structure-american-economy-employment-challenge/p24366 (accessed April 9, 2014).
- Stafford, M., T. Chandola, and M. Marmot. 2007. Association between fear of crime and mental health and physical functioning. American Journal of Public Health 97:2076–2081. https://doi.org/10.2105/AJPH.2006.097154
- Steptoe, A., and P. J. Feldman. 2001. Neighborhood problems as sources of chronic stress: Development of a measure of neighborhood problems and associations with socioeconomic status and health. Annals of Behavioral Medicine 23:177–185. https://doi.org/10.1207/S15324796ABM2303_5
- Sum, A., I. Khatiwada, J. McLaughlin, and S. Palma. 2009. The consequences of dropping out of high school: Joblessness and jailing for high school dropouts and the high cost for taxpayers. Boston: Center for Labor Market Studies, Northeastern University. Available at: https://www.issuelab.org/resource/the-consequences-of-dropping-out-of-high-school-joblessness-and-jailing-for-high-school-dropouts-and-the-high-cost-for-taxpayers.html (accessed May 28, 2020).
- Taras, H., and W. Potts-Datema. 2005. Chronic health conditions may also impact children’s development and educational performance. Journal of School Health 75(7):255–266. https://doi.org/10.1111/j.1746-1561.2005.00034.x
- Thoits, P. A. 2010. Stress and health: Major findings and policy implications. Journal of Health and Social Behavior 51(Suppl.):S41–S53. https://doi.org/10.1177/0022146510383499
- University of Wisconsin Population Health Institute. County Health Rankings 2013. Available at: www.countyhealthrankings.org (accessed June 3, 2014).
- U.S. Census Bureau. 2012. American Community Survey, 2009–2011. Detailed tables using American FactFinder. Available at: http://factfinder.census.gov/home (accessed December 12, 2012).
- U.S. Census Bureau. 2013. Public education finances: 2011. G11-ASPEF. Washington, DC: Government Printing Office. Available at: https://www2.census.gov/govs/school/11f33pub.pdf (accessed May 28, 2020).
- Weisleder, A., and A. Fernald. 2013. Talking to Children Matters: Early language experience strengthens processing and builds vocabulary. Psychological Science 24(11):2143–2152. https://doi.org/ 10.1177/0956797613488145
- Willems, S., S. De Maesschalck, M. Deveugele, A. Derese, and J. De Maeseneer. 2005. Socio-economic status of the patient and doctor-patient communication: Does it make a difference? Patient Education and Counseling 56:139–146. https://doi.org/10.1016/j.pec.2004.02.011
- Williams, D. R., and S. A. Mohammed. 2009. Discrimination and racial disparities in health: Evidence and needed research. Journal of Behavioral Medicine 32(1):20–47. https://doi.org/10.1007/s10865-008-9185-0
- Williams Shanks, T. R., and C. Robinson. 2013. Assets, economic opportunity and toxic stress: A framework for understanding child and educational outcomes. Economics of Education Review 33:154–170. Available at: http://www.sciencedirect.com/science/article/pii/S0272775712001458 (accessed June 3, 2014).
- Wilson, J. W. 1987. The truly disadvantaged: The inner city, the underclass, and public policy. Chicago: University of Chicago Press.
- Winkleby, M., C. Cubbin, and D. Ahn. 2006. Effect of cross-level interaction between individual and neighborhood socioeconomic status on adult mortality rates. American Journal of Public Health 96:2145–2153. https://doi.org/10.2105/AJPH.2004.060970
- Zhang, T. Y. and M. J. Meaney. 2010. Epigenetics and the environmental regulation of the genome and its function. Annual Review of Psychology 61:439-466. https://doi.org/10.1146/annurev.psych.60.110707.163625
https://doi.org/10.31478/201406a
Suggested Citation
Zimmerman, E. and S. H. Woolf. 2014. Understanding the Relationship Between Education and Health. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201406a
The views expressed in this discussion paper are those of the authors and not necessarily those of the authors’ organization or of the Institute of Medicine. The paper is intended to help inform and stimulate discussion. It has not been subjected to the review procedures of the Institute of Medicine and is not a report of the Institute of Medicine or of the National Research Council.
Join Our Community
Sign up for nam email updates.
- Skip to main content
- Skip to secondary menu
- Skip to primary sidebar
- Skip to footer
A Plus Topper
Improve your Grades
Essay on Health | Health Essay for Students and Children in English
February 12, 2024 by Prasanna
Essay on Health: The World Health Organization defines health as a state of mental, physical, and social well-being, and not merely physical well-being. Individuals who are healthy in mind are automatically healthy in their bodies. Good health is man’s greatest possession. A healthy person is one who can function up to his optimal capacity without any difficulty. Good health facilitates a lot of other body processes. Good health helps us to handle stress and combat with increasing pressures.
To help students in writing academic essays and give speeches, we have provided long and short essays on health in this article. We have also added ten lines about fitness so that children can easily take part in competitions and win prizes.
You can read more Essay Writing about articles, events, people, sports, technology many more.
Long and Short Essays on Health for Students and Kids in English
Given below is one brief essay on health, consisting of 500 words and one short essay of 100-150 words.
Long Essay on Health in English 500 words
Essay on Health is usually given to classes 7, 8, 9, and 10.
The world is going through rapid changes, and the only constant thing that is in our hands is our health. Being healthy is a choice. Specific guidelines are there to maintain good health, but in the end, it is individual effort and determination. Good health is essential for having a pro-active and fully functioning life. Man is a social animal, and good health ensures social survival. Health, besides being personal, is also social. A healthy person can bring positive changes in society. It is not an end to itself but also the key to creating a better and more reformed community.
Health can be of varied types; physical, emotional, mental, social, spiritual, and sexual health is some of them. Distress can cause neurotic disorders, and healthy people are less likely to fall prey to them. Physical health refers to the bodily well-being of individuals. It involves maintaining a healthy lifestyle. An individual who follows a balanced diet, replenished with carbohydrates, proteins, fats, vitamins, and minerals, in adequate quantities, usually has better immunity. Health is Wealth means good health is the real treasure. A healthy life enables one to remain positive and face all life challenges.
Physical health requires few dedicated efforts, including regular exercise and consumption of a lot of water. Water regulates all our body processes, reduces chances for zits and pimples, and ensures regular bowel movements. Exercises like brisk walking, running, cycling, and skipping help in maintaining proper body weight.
Even if an individual has specific issues like heart diseases, he must know the required guidelines. The guidelines involve not eating very oily food, avoiding junk food, and so on. A diabetic person must adhere to the doctor’s instructions and consume minimum sugar. Children should eat more proteins as they are body-building nutrients. Physical health is essential for a long and pleasant lifespan.
Mental health refers to our emotional and psychological well-being. Mental health has a significant impact on our thoughts, behaviors, and attitude. It is essential to give equal attention to our mental health as its effects are grave. Society has a significant impact on an individual’s mental health. Societal pressures about getting jobs and getting significantly married affect our peace of mind. In addition to false standards of beauty imposed on us, harmful and hurtful remarks regarding someone’s body and various unnecessary criticisms take a toll on our mental health.
Teenagers are very susceptible to depression and anxiety as they go through the troubled adolescent period. Adults expect them to take up responsibilities all of a sudden, and they cannot cope up with their expectations. Hence, they suffer from an identity crisis as they cannot comprehend the roles that they should play.
Adolescents often fall under peer pressure and take to bad habits like drugs, alcohol, which makes them unfocused. Retired individuals also suffer from loneliness and depression as they feel that they have lost their prominence in the family. Heavy workload and pressure to meet deadlines, merged with an unhealthy workplace environment may also affect mental health.
It is essential to create a positive environment around yourself to counter the negativity. Cutting off toxic people is the right way of having better mental health. Above everything, we must choose happiness and optimism as the guiding principles of our life.

Short Essay on Health in English 150 words
Essay on Health is usually given to classes 1, 2, 3, 4, 5, and 6.
It is healthy to start by taking a simple resolve that we will love and care for ourselves. There are few fixed ways of maintaining good health, but it is a subject that demands maximum exploration. Individuals have varied needs, and thus, different measures might work for different people. Starting each day with some free-hand exercise like jogging or running ensures proper blood circulation in the body.
Yoga can be a very healthy way of taking your mind off hectic schedules and focus on your spiritual transcendence. One must consume meals at regular intervals and not skip meals, which leads to indigestion and weight gain. Most importantly, keeping a part of your day as “me time” will help to reduce stress. Being healthy facilitates our productivity and ensures that we lead fulfilling lives.
10 Lines on Essay on Health in English
- Health is a state of physical, mental, and social well-being and is very important for success and survival.
- It is essential to be healthy as it affects our productivity and performance.
- Adolescents who struggle with meeting expectations often face mental health issues. The only way of solving it is to talk to them and help them understand their roles.
- Toxicity in the environment can harm a person’s health to a great extent. It is essential to create our safety circles and vent our innermost thoughts.
- A healthy lifestyle includes eating healthy and consuming green leafy vegetables, fish, meat, and eggs that are high in protein and minerals to help in maintaining good health.
- Water is an essential portion of our diet and helps in every biological process. Drinking water ensures clearer skin.
- Choosing optimism helps in having stable mental health. One must do what he likes to do and thrive in his sphere.
- Creative get-away like painting, drawing, listening to soothing music, help in being healthy.
- A proper sleep schedule with a minimum of 8 hours of sleep is essential for being healthy.
- Regular check-ups help in preventing grave illnesses and ensure good health.
FAQ’s on Essay on Health
Question 1. What are some ways of being healthy?
Answer: Ways of being healthy to include following a balanced diet, going for regular check-ups, and maintaining a proper sleep schedule.
Question 2. What are some interesting health facts?
Answer: Laughing is a perfect way of regulating blood circulation. Laughter therapy helps in controlling anger and having better mental health.
Question 3. What is social health?
Answer: Social health involves having a positive atmosphere around you and being with those who make you genuinely happy and inspire you.
Question 4. Can mental health affect our physical health?
Answer: Yes, people suffering from depression often have insomnia, and the lousy sleep schedule takes a toll on their health.
- Picture Dictionary
- English Speech
- English Slogans
- English Letter Writing
- English Essay Writing
- English Textbook Answers
- Types of Certificates
- ICSE Solutions
- Selina ICSE Solutions
- ML Aggarwal Solutions
- HSSLive Plus One
- HSSLive Plus Two
- Kerala SSLC
- Distance Education
Essay on Health Education in English for Children and Students

Table of Contents
The term “Health Education” refers to a profession wherein people are taught about the promotion, maintenance and restoration of their health. Health in this aspect refers to mental health, physical health, psychological health, social health, sexual health and reproductive health. The World Health Organization (WHO) defines Health Education as a program to improve health literacy and develop skills which are conducive to individual and community health.
Fill Out the Form for Expert Academic Guidance!
Please indicate your interest Live Classes Books Test Series Self Learning
Verify OTP Code (required)
I agree to the terms and conditions and privacy policy .
Fill complete details
Target Exam ---
Long and Short Essay on Health Education in English
Below we have provided Health Education essay of varied lengths, covering all the significant aspects of health education. You can choose any of the essay on Health Education as per your requirement. You can use them for essay writing competition or presentation in your school/college or elsewhere.
Health Education Essay 1 (200 Words)
In a lay man’s term, Health Education is defined as a program which teaches an individual or a community about the methods to improve their health conditions by providing health literacy. Health Education covers various aspects, ranging from social health, mental health to sexual and reproductive health.
Every year, millions of lives are lost globally because of infectious diseases, and other causes due to the lack of health education and general public awareness. The situation is more critical in developing countries where high mortality rate of infants exists due to lack of basic health amenities and low public awareness. In India diseases like diarrhea, infections of lower respiratory tract and other communicable diseases, constitute the prime causes of infant mortality. Health Education; therefore, becomes a necessity to raise the literacy level of people in areas concerning health and hygiene of self, as well as that of community.
However, the average life expectancy by birth in India has increased from 49.7 years in 1970-75 to 69.1 in 2018, due to the government’s efforts in promoting health education through a well trained and equipped staff. Also the infant mortality rate has nearly halved to 34 per 1000 births, since the past decades.

Health Education Essay 2 (300 Words)
Introduction
“Health Education” refers to educating an individual or a community for adopting better, healthy and hygienic living conditions. Health Education aims to raise awareness of individuals and communities on various aspects of health like – physical health, mental health, psychological health, prevention of diseases, sexual and reproductive health etc. Health education is a broad subject and might also include topics like health issues of alcohol, drugs, tobacco and environmental health.
Who are Health Educators
Anyone with proper knowledge of health and hygiene and relevant knowledge on health issues could provide health education through face to face interaction with individual or community. However, some people are especially trained for the purpose and are certified health specialists, also referred to as health educators.
The government of India has launched a number of programs for promoting health care, preventing communicable – non communicable diseases and other relevant causes. The programs have a dedicated team of trained professionals functioning as health educators and medical supervisors. Health educators interact with villagers in remote areas, educating them on the issues of general health and diseases.
Teachers in schools could also function as health educators by educating children about maintaining proper health and hygiene. They can educate children about various communicable and non communicable diseases and how to prevent them by adopting health habits and hygiene.
Health Education in developing countries is an absolute necessity, in order to raise health literacy and lower the mortality rate arising due to various diseases and other health related issues. There is also a need for mandatory health education in schools by making the necessary policy changes in this regard. The authorities must also ensure that the program is backed up by a trained workforce, specializing in interacting and educating children and teachers. Also the teachers could be trained as health educators, to spread awareness among the students and community.
Health Education Essay 3 (400 Words)
Health Education refers to educating individuals, groups or communities in areas of health. It aims to educating people on how to maintain personal health. However, in broader aspects, health education also aims to improving the overall health of a community. It also covers various areas of health as – physical health, mental health, psychological health, emotional health, sexual health and reproductive health.
State of Health Education in India
The need for public health education in India was realized as early as in 1940, when a committee under the chairmanship of Sir Joseph Bhore (Indian Civil Servant) emphasized on the inadequate teaching on public health in undergraduate training programs for medical students.
Today health education in India has been considerably improved, backed by various institutes and a trained workforce including doctors, nursing workers paramedics etc who specialize in areas of public health.
Presently, India has two types of public health professionals – one who is trained in core public health or specializes in a specific public health area; second, who acquire a medical degree or diploma before specializing in public health.
Though, the state of health education in India is constantly improving because of various government initiatives to improve and increase trained workforce; still, there is a shortage of trained professionals and a need to increase their numbers and skills.
Role of Health Educator/Teacher in Health Education
The spread of diseases and subsequent deaths could best be prevented by educating people on the various areas of health education. Here comes the role and need for a health educator. A health educator is a professionally trained individual who specializes in areas regarding public health. He is well equipped with resources and strategies to educate individuals, groups or communities on how to maintain proper health and hygiene. School teachers are also trained in areas public health under various programs, in order to increase the workforce and to reach out to more and more people.
Despite all the institutes that provide professional courses on public health, there is a shortfall of trained public health work force in India. There is a need to set up more institutes and including professionals from other fields in order to fill the gap. Also, the number of students opting for public health is considerably low with regards to other professional degree or diploma courses. Thus, for improving public health, we need to build institutes giving public health professionals, create job opportunities for those professionals and framing a career path for them.
Health Education Essay 4 (500 Words)
Health Education constitutes educational programs directed towards improving the state of health and hygiene among individuals and communities. Health Education provides information about the factors that affect the health and hygiene of an individual or a community.
Strengths of Health Education in India
One of the main strengths of Health education in India is the presence of an adequate multi level infrastructure both in the government and non government sectors. The central health education bureau works in collaboration with the state health education bureau, up to the block level.
Another strength of Health education in India is an efficiently trained work force. Majority of health educators in India are either graduate or post graduate.
Another strength of health education in India lies in the successful information dispensation throughout its states, despite the linguistic variations. India has 15 official languages and several local dialects; even then health education programs are able to successfully convey the message.
Weaknesses of Health Education in India
Weaknesses of the health education in India include high dependability on print media, lack of research and conventional training methods of educators, inability to reach all the remote villages and no avenues of professional growth for health educators.
Most of the campaigns on health education, either in government or non government sector rely on print media for promotion; through, newspapers, posters and pamphlets. Around 40% of Indians are unable to read or write, which defeats the purpose as the promotion fails to reach the uneducated at ground level.
Another weakness of Health education in India is the absence of better growth avenues for the functionaries. Because of not being properly organized, the profession is non lucrative for youths, who rather opt for other more promising professional courses.
Also, the mode of training and education in public health is conventional and there is a dire need to integrate modern techniques along with better exposure to the professionals.
Methods to Improve Health Education in India
One of the best ways to improve the state of public health education in India is to let a well trained workforce reach out to people in remote areas. More emphasis should be given on interacting with the villagers on occasions of public gathering like – fares, markets etc. Moreover, methods like plays, folk shows should be used to convey the message, rather than print media.
People visiting hospitals and clinics are more conscious about health issues and so efforts must be made to educate them. They naturally tend to be more receptive and benefit from the programs.
Schools could also play a significant role in spreading health education. Schools are the best place to interact with children belonging to different sections of society. Teachers could be adequately trained to impart health education to the children. Children on the other hand could share their knowledge with their parents, relatives and friends.
Also it should be made compulsory for any medical professional to serve a fixed tenure in some remote village, where s/he is vested with the responsibility of educating people about health and hygiene along with addressing their ailments.
It is imperative for India to improve to a never seen before standards of health. For which it also necessary to target the marginalized sections of Indian society; for it is them who are deprived of basic health amenities and are oblivious of many health concerns. There is a need to open new avenues of health education, at ground level as well as strengthening the infrastructure related to health education.

Health Education Essay 5 (600 Words)
“Health Education” aims to impart knowledge regarding measures to be taken by an individual or community in order to improve their overall health. India is a developing nation, but various communicable and non communicable diseases still claim thousands of lives annually. Also, the figures reveal varying infant mortality rates from states to states – it is 6 per 1000 births in Kerala and in Uttar Pradesh it is 64 per 1000 births.
The prime cause of high infant mortality is the absence of trained medical professionals and people’s own ignorance about health conditions. In such state of affairs, it becomes imperative for India to have an effective infrastructure backed by equally effective work force to address to the medical needs of people and also to raise their level of health education and literacy.
Importance of Health Education
Health education improves the status of overall health of an individual and community, ultimately resulting in a better overall health of the nation. Health education is directly related to a nation’s economical growth, as a better health education results in high life expectancy and a raised standards of living.
Who Provides Health Education
Health Education is provided by trained professionals known as – health educators. They are certified specialists holding a certificate in public health or on a specific health issue. The work force of Public health education constitutes of doctors, paramedics and the nursing staff. They are trained in areas of health and hygiene and also are well equipped with necessary resources to reach out to people and educate them. Many professionals from different fields too, volunteer to provide health education to masses after going a required amount of training.
Motive of Health Education
Health education aims at improving the health condition of an individual and a community. It teaches an individual the ways to stay healthy and remain safe from diseases. It also aims at developing in them a sense of responsibility towards themselves as well as towards the community.
Health education is very significant in developing nations. It imparts to the people, the basic health knowledge about health and hygiene, by shaping their day to day activities. Moreover, other than physical health, health education also aims for addressing other serious issues like stress, depression or other emotional disturbances.
India’s Stand on Health Education
In the recent years there has been an increasing trend in non medical professional institutes in India, offering public health programs to the students. Today around 23 institutes in India today offer Master in Public Health with annual enrollment of 573 candidates.
School Health Program was launched by the Government of India in 2009, with aim of addressing to the health needs of school going children. The program not only caters to the physical well being of school going children but also to their emotional, psychological and nutritional needs. Every year huge funds from centre and states are allocated for the programs which benefit millions of students from marginalized sections of the society.
The Pradhanmantri Swasthya Suraksha Yojna (PSSY) was also launched in 2003, with the aim of making tertiary healthcare services affordable to the masses and also to improve the quality of medical education.
Despite various government programs regarding improving and promoting quality of health education in India, many still don’t have access to basic healthcare services and are out of the reach of public health educators, due to the lack of necessary infrastructure at ground level. Many programs which aimed at raising public awareness about AIDS, cancer, malaria etc, failed to build the necessary infrastructure at the grass root level. In order to make health education in India a success, there is a need for adequate infrastructure and well trained and equipped work force.
Related Information on Hindi
Related content

Get access to free Mock Test and Master Class
Register to Get Free Mock Test and Study Material
Offer Ends in 5:00
Select your Course
Please select class.

Mental Health: What Works?
How colleges and universities are rising to the challenge of supporting students emotionally and psychologically
Summer 2024
It takes a student with the will to confront a difficult problem. It takes a friend who offers encouragement, a faculty member who provides guidance, a counselor who offers assistance. It takes courage, compassion, and strength.
The need for this campus-wide support network has never been higher. Seventy percent of students say they have struggled with mental health issues since starting college, a March 2024 U.S. News /Generation Lab survey found. In the 2022–23 Healthy Minds Network’s annual student survey, 41 percent of college students screened positive for major or moderate depression, 36 percent screened positive for major or moderate anxiety, and 14 percent said they had seriously considered suicide.
Another statistic, however, offers hope. The number of students participating in counseling increased from 30 percent to 37 percent between 2020 and 2022, according to a study of Healthy Minds survey data. Students are seeking aid—and campuses are rising to the mental-health moment. Here are some ways that they are helping students with emotional and psychological challenges ranging from building resilience to coping with grief.

Stories of Adversity and Strength
Emory University Atlanta, Georgia
Enku Gelaye came to the United States from Ethiopia when she was seven. She studied engineering in college to fulfill her father’s wishes but sought a different path. Kristina Bethea Odejimi was a student-athlete who injured her right knee in high school, then injured the left one as a college senior, ending her basketball career. Munir Meghjani was on the debate team in high school, but at his first tournament, he had to race to the bathroom with an upset stomach. The problem resurfaced for months when he tried to debate.
What do these people have in common? Each faced challenges, each overcame them, each saw it as a turning point in their lives—and each is a staff member, faculty member, or alumnus of Emory University. Gelaye defied her family’s expectations by trading engineering for a journalism degree. She is now senior vice president and dean of campus life. Odejimi’s basketball career ended, but she learned that “my sport was a piece of my identity and not my total identity.” Today, she is associate vice president for belonging, engagement and community and dean of students. Meghjani slowly summoned the “grit and resilience that I was taught by my family and my community” and overcame his fears to become a top high school debater. He is a commercial real estate agent and past president of the Emory alumni board.
Emory’s Campus Life Office collected all three of their stories for a project called “Reframes: Discovering the Possible.” The idea: to show how various faculty, staff, and alumni reframed life’s unexpected detours and embraced change. In the student centers at Emory’s Atlanta and Oxford campuses, a series of black-and-white portraits show Reframes participants. Next to each photo is another black-and-white shot, this one of a participant’s hand holding a card that reveals lessons learned from the participant’s mistakes. A QR code takes viewers to three-minute videos in which the participants—from an executive associate dean whose son was an addict to an associate dean who got divorced—share a personal crisis and how they coped. Videos are also shared via Emory’s social media accounts and email communications (you can find videos at reframes.emory.edu ).
A key Reframes message is that challenges and self-doubt are inevitable. “We don’t succeed by being perfect,” Emory President Gregory L. Fenves says in a video. “You grow through experience, by making mistakes, learning, and allowing yourself time and grace.” That’s an important statement at colleges and universities like Emory, where high achievers often feel enormous self-pressure to succeed, points out James Raper, associate vice president for health, well-being, access, and prevention at Emory.
“They’ve gotten really good outcomes from that, but it’s not sustainable,” Raper says. “It’s often in college or university where [students] realize, ‘This approach isn’t working for me’—the rigid, toxic perfectionism that they approach their lives with.”
It’s not just fear of failure. It’s fear of being average. Students at Emory, Raper has found, abhor a “C” more than an “F.”
“Every time I say that to a student group, they all kind of groan and nod,” he says. “A ‘C’ is the worst. It’s the seeds of mediocrity that they really fear.”
In addition to the videos, Reframes creates opportunities to discuss those anxieties via in-person events. During the spring 2024 semester, the Campus Life Office hosted small-group dinners, from a picnic on a campus lawn to meals in private dining rooms at the student centers, where students were able to talk with faculty and staff about life’s hurdles and failures. Campus Life also sets up an on-campus photo booth where students can share their own stories.
These efforts help address another issue: loneliness. Emory’s student well-being surveys consistently show high loneliness numbers. The Reframes activities help combat that by building connections and a sense of belonging on campus.
“We’re creating lots of opportunities for students to practice connecting with one another in a more authentic way,” Raper says.
Raper, too, has embraced that authenticity. He appears in one of the Reframes videos in which he shares his own collegiate setback.
“I got kicked out of college academically, and I had mental health issues,” he says. “I was very fortunate to get back into that university.” Raper has told that story over the years to show students that their lives won’t end if they fail. And as he and his colleagues have shown through Reframes, failure is often not an ending but a beginning.
A Student Well-Being Committee
If you want to improve students’ well-being, shouldn’t they have a say in what they need? That thinking led James Raper, associate vice president for health, well-being, access, and prevention, to form the Student Well-Being Advisory Committee (SWAC) at Emory shortly after he was hired in 2022. The committee—a mix of undergraduate and graduate students—meets at least monthly through the academic year and provides input on well-being strategies, programming, and more. SWAC helped develop the “Reframes: Discovering the Possible” project, suggesting candidates for interviews (committee members wanted to hear from university faculty and leaders) and offering feedback on the project’s look and feel. The committee recruits members via word of mouth; recommendations from staff, faculty, and peers; and recruitment emails and social media posts. “We can’t be making decisions for our students and guessing what’s going to work,” says Raper, who also meets individually with members. “The committee really informs me and my team.”
Eating Disorders

A Partnership to Save Lives
Texas Christian University Fort Worth, Texas
For psychologist Amanda Swartz and her colleagues, the numbers were frightening. Between 2019 and 2022, the Texas Christian University (TCU) Counseling and Mental Health Center had seen a 442 percent increase in eating concern and body image appointments. The center had an eating disorder team, which included a certified eating disorder specialist and supervisor, but Swartz and the other staff knew they needed to strengthen their services. They contacted the Eating Recovery Center (ERC) and established a unique partnership to provide an in-person, on-campus intensive outpatient program for students.
“This is very rare,” Swartz says of the partnership, which launched in August 2023. “We are hoping to use our experience to provide education and training to other schools.”
Headquartered in Denver, the ERC provides therapy at thirty-five centers in seven states, with virtual programs in eight other states. The intensive outpatient program helps students with severe symptoms or long-term issues, including the three most common eating disorders: anorexia (having a low body weight and using severe methods to shed pounds and limit calories), bulimia (which includes periods of bingeing followed by purging), and binge-eating disorder (in which bingeing is followed not by purging but feelings of guilt, shame, or revulsion).
The intensive outpatient program at TCU is identical to those at the ERC’s own facilities. Students who enter the program attend a three-hour group session three times a week, along with weekly individual sessions with a therapist and a dietitian. The average time in the program is about eight weeks.
TCU chose the ERC because it’s a nationally recognized leader in eating disorder treatments, it has a location in Dallas (about thirty-five miles away), and it was willing to tailor the days and times of the sessions to best meet students’ schedules. This allows students to access care and continue their studies while participating in treatment.
“A key point of having the program is that they remain in school. This gets rid of the difficulty of driving to Dallas, which adds an extra two hours onto their treatment day,” Swartz says. “It also puts them with other TCU peers, and it allows them to get treatment in a familiar setting. It doesn’t seem quite as scary because even though it’s a different program, it’s still in our counseling center, it’s still on their campus, but they’re able to get that higher level of care that they need.”
A growing number of students nationwide need treatment. From 2013 to 2021, the risk of developing an eating disorder jumped from 15 percent to 28 percent among US college students, according to a study of Healthy Minds survey data. During the pandemic, eating disorders among teens nearly doubled, a study in JAMA Pediatrics found.
Many types of students can be susceptible to eating disorders. Some are overachievers and perfectionists. Others have been sexually abused. Some fall into both categories. Whether they’re binge eating or suffering from conditions such as anorexia, many are seeking a type of emotional numbing, experts say. Genetics can also be a factor.
“There’s actually a huge genetic component to eating disorders,” says Landry Weatherston-Yarborough, ERC executive director of the south region, who helped open the facility at TCU. “It’s one of the most inheritable mental health diagnoses, second only to autism spectrum disorder.”
Although eating disorders can start in childhood, college students are often vulnerable because they’re undergoing a major life transition.
“So many of them are moving away from home for the first time, living independently, managing their own schedules,” Weatherston-Yarborough says. “They may have new financial stressors. Maybe they’re holding down a job as they’re going to school, dealing with roommates. Those are traditionally vulnerable times for an eating disorder, even if someone never had one before. And the hard thing about eating disorders is that people often feel in control when they’re engaging in those behaviors, but the eating disorder actually has the control.”
The intensive outpatient program is helping students develop the tools to regain that control and rebuild their lives. The partnership is only one year old, so the counseling staff is still collecting data, but “it seems that the students who went through the program had good outcomes. I’ve had students tell me they wouldn’t have graduated if they hadn’t had eating support on campus,” Swartz says. “And some say they don’t think they’d be in recovery if they hadn’t gotten treatment.”
Mental Health First Aid

An Awareness of when People Need Help
University of North Carolina Chapel Hill, North Carolina
Sam Deal had noticed an occasional bandage on his colleague’s hand. The coworker claimed it was a burn injury from a cooking mishap, but the wound kept recurring. Deal, a facilities manager in the School of Social Work at the University of North Carolina (UNC) at Chapel Hill, suspected self-harm and that the bandage was a cry for help.
Deal’s suspicions were informed not only by personal experience with a family member but also by his training in Mental Health First Aid (MHFA), a course that teaches faculty, staff, and students how to “identify, understand, and respond to signs of mental illnesses and substance use disorders.” Developed by the National Council of Mental Well-Being, the MHFA course is offered by the School of Social Work’s Behavioral Health Springboard (a program that provides health-related programming and assists other organizations with programming). Instructors, who receive training from the National Council for Mental Wellbeing, include UNC-Chapel Hill staff and faculty in the School of Social Work, School of Nursing, School of Pharmacy, School of Education, and School of Medicine.
Not long after receiving training, Deal invited the coworker to lunch, followed by a walk, and shared his concerns.
“The floodgates opened,” he says of his colleague’s response. The coworker had struggled for years with emotional and physical abuse, and the self-inflicted burns were an attempt to mask the internal pain. After their talk, Deal contacted his MHFA coordinator, who quickly shared free county and state resources (coordinators help with the logistics of offering the MHFA course). Deal’s coworker accepted the assistance, began seeing a counselor, and is now thriving professionally and personally.
UNC-Chapel Hill has offered the course since 2015; more than a thousand faculty members, staff, and students voluntarily participated in 2022 alone. Some enroll individually, while others participate as part of a group: the UNC-Chapel Hill library staff, for example, underwent group training. Library staff observe numerous students during their workdays; the training might help them to spot students who are struggling emotionally. Once participants complete the course, they are certified in MHFA for three years (and they can retake the course to become recertified).
Participants learn a variety of mental health warning signs (for example, changes to typical behaviors, such as increased sleeping and decreased eating) along with “how to approach people and how to respond and what resources you can recommend,” says Alicia Freeman, the MHFA program manager at UNC-Chapel Hill and a licensed clinical mental health counselor and addictions specialist. Many participants say that MHFA has not only helped them identify students and colleagues struggling with mental health issues but also family members and even strangers.
“I’ve had faculty and staff say that since COVID, it just seems like everybody is under more stress and experiencing more mental health [challenges],” Freeman says. “People want to be informed and better equipped to support the community.”
The course begins with two hours of self-paced online work, followed by five and a half hours of live course sessions. Some sessions are virtual, others are in person, and they’re available throughout the week, including evenings and Saturdays. That flexibility helps students juggle the training with classes and extracurricular activities. Zoe Anne Biebesheimer, a senior majoring in human development and family science, took the training in 2023. It was required for a student organization called LSN (Listen, Support, Navigate), a peer group that monitors chats on the Heels Care Network, a UNC-Chapel Hill mental health website.
“It was a great way to build my confidence in terms of how to approach certain situations and how to begin certain tough conversations regarding mental health challenges,” says Biebesheimer, who’s interested in becoming an MHFA instructor. “The training was helpful in giving me a baseline for assessing risk and assisting peers.”
Deal is equally enthusiastic. Since receiving his initial instruction in 2016, he has twice retaken the course to remain certified.
“Each time, I’ve learned something new and taken away a better understanding of the mental health challenges that so many in our society deal with,” he says. “Had it not been for this training, I might have never given a second thought to the recurrence of my colleague’s injuries.”

Well-Being in the Classroom
Georgetown University Washington, District of Columbia
At the start of each semester, associate biology professor Heidi Elmendorf shares information with her students that goes far beyond the syllabus. She tells them about her struggles with depression, and sharing that vulnerability, she believes, changes the dynamics of her course, Foundations in Biology. Instead of a detached, me-and-them, professor-and-student relationship, she says, the class becomes an “us.” Elmendorf then asks students to take an anonymous mental health survey, the results of which guide the semester’s discussions and students’ research paper topics. As she notes in the course description, Elmendorf hopes the class gives students “a sense of comfort as a community” and “unexpected resources for coping.”
If this doesn’t sound like a standard undergraduate biology course, there’s a reason: it’s not. Foundations in Biology is an Engelhard Course, which is part of Georgetown’s Engelhard Project for Connecting Life and Learning. Supported by an endowment from the Charles Engelhard Foundation, the project’s primary function is to help integrate well-being topics in courses across the university to connect “students’ academic studies and their broader life experiences, especially in the areas of well-being, flourishing, and mental health.” The result: students feel that courses are more relevant to their lives and engage more with course material.
Since 2005, more than 20,000 students have taken an Engelhard Course, and close to 220 faculty members and 95 campus resource professionals have participated in 650 courses. When the program started, Georgetown offered five Engelhard Courses. In the spring 2024 semester, the university offered fifty-eight.
Each semester, faculty apply with the Engelhard Protect to be fellows and submit course proposals. Among the proposal requirements: each course must feature an in-class visit from a Georgetown campus resource professional, such as a staff member from the student health center or the LGBTQ+ resource center. Course subjects range from psychology to ethics and even math. One example of an Englehard Course is Introduction to Math Modeling, which incorporates data sets involving nutrition, gambling, and alcohol. Other examples are Art of the Monologue, which features discussions of mindfulness, and an intro-to-ethics course that teaches Immanuel Kant’s writings on topics like substance abuse and sexual objectification. Georgetown’s associate director for sexual assault response and prevention services gives a guest lecture to “bring campus life into the classroom,” as the course description states.
Not all courses work as an Engelhard Course. But in those that do, instructors say, students often have an easier time learning the subject matter and enjoy a deeper relationship with professors.
“One faculty member said to me that ‘Engelhard has helped me see my students as whole people and bring more of my whole self to the course and to my teaching,’ ” says Joselyn Schulz Lewis, co-lead for the Engelhard Project for Connecting Life and Learning and senior associate director for inclusive teaching and learning initiatives at the Center for New Designs in Learning and Scholarship. “ ‘When I do that, I enjoy it more. I think they’re learning better. I think I’m teaching better.’ ”
Students often don’t realize they’re taking an Engelhard Course, yet for many, the impact can be profound. Nestory Ngolle is a pre-med junior who took an Engelhard Course called Introduction to Medical Anthropology, which changed his thinking about patient care.
“The professor aimed to break that mold of what we think of as health care and reshape it in a form that essentially targets a patient’s needs,” says Ngolle, who serves on Engelhard’s student advisory council. “If someone has a cold, maybe they need NyQuil to feel well physically. But maybe they would feel mentally well if they could take the day off and rest. Those are two different kinds of wellness. And being in a class that recognizes those differences, and illuminates them. . . . I found that to be a great experience with the Engelhard project.”
For faculty like Elmendorf—who before the Engelhard project hadn’t revealed her depression—the experience has been equally transformative. You cannot “legitimately invite your students into this space if you’re not willing to join them in this space,” Elmendorf says in a video on the Engelhard website (engelhard.georgetown.edu). “To understand that a faculty member is also struggling with mental health issues . . . instantly changes their perception about who our community is and who they can be.”
Indigenous Teachings for Healing
Diane Schenandoah is a Syracuse University (SU) alumna. She’s also a faith keeper (someone who oversees her peoples’ spiritual well-being) of the Wolf Clan of the Oneida Nation, which is part of the Six Nations Haudenosaunee Confederacy. And she is the first to serve in the role of Honwadiyenawa’sek, a Haudenosaunee word for “one who helps them,” at the university. Syracuse is located on the ancestral lands of the Haudenosaunee Confederacy—also known as the Iroquois Confederacy, which includes the Cayuga, Mohawk, Oneida, Onondaga, Seneca, and Tuscarora peoples—and the university has committed to “empowering and supporting Indigenous students of any tribe or nation.” That included hiring Schenandoah in 2021 as a part-time employee in the SU counseling center. Schenandoah is available to any students seeking her support and uses traditional energy work practices, including acupressure, art therapy, and tuning forks (the vibrations are supposed to balance the body’s circadian rhythms) to help students feel more centered, balanced, and grateful. “We’re all creative beings, and we need to give thanks for all things that surround us,” she explained in an interview for an SU podcast. “It’s really rewarding to see the students’ faces light up when they discover their own inner strengths and their own energy.”
Grief and Loss

An Understanding That It’s Not Just about Death
University of Indiana South Bend South Bend, Indiana
The University of Indiana (UI) South Bend’s Student Counseling Center recognizes that grief, loss, and trauma can result from more than the death of a loved one. They can also stem from life challenges such as divorce, unemployment, and even academic disappointments.
“It is not uncommon for a medical school student to come in and say, ‘I’ve never had anything below an A minus in my entire academic career, and now I haven’t passed an exam,’ ” says Kevin Griffith, associate vice chancellor for student engagement. “All of our populations face academic hurdles and challenges, and grief, loss, and trauma therapy can help them navigate it.”
Grief, loss, and trauma can also involve financial insecurity.
“About one-third of college students on small regional campuses such as ours, which serve a number of underrepresented students, will experience food insecurity while they are in college,” Griffith says. “And about 8 percent of those students will face homelessness at some point during their undergraduate experience. So grief, loss, and trauma include all kinds of loss.”
The counseling center provides everything from one-on-one sessions with counselors (who are certified in grief, loss, and trauma) to community workshops. The goal of the offerings: “to get a conversation going on grief, loss, and trauma and to help students and community members break down the stigma of asking for help when it comes to mental health,” says Griffith, who oversees the Office of Veteran Student Services and the Office of Accessible Educational Services in addition to the counseling center. “The populations that we support—veterans and people with disabilities, as well as our general population of students—experience a great deal of loss and trauma.”
The counseling center also works with local nonprofits and government agencies, as well as individuals in private practice, to provide students with grief-and-loss services such as pet therapy and art and music therapy. The intent, Griffith says, is to “introduce holistic support through the therapeutic process” and offer services beyond what counseling centers usually provide.
Confronting grief is important for students, not just personally but academically, whether they’re mourning the death of a loved one, a breakup, or the loss of a scholarship, Griffith has found.
“It’s an extra level of pressure and stress that students are feeling,” he says. And sometimes students are coping with death, often for the first time. Some may have lost a grandparent who helped raise them. Others, particularly those from underrepresented communities, may have lost a friend to violence. Encouraging these students to seek help involves a simple message: it’s OK to seek help. The counseling center delivers that message through classroom presentations, workshops, discussions, and marketing campaigns and by engaging with student groups, student leaders, faculty, and staff. One campaign, called “Unboxed: Open Up about Mental Health,” encourages students to “overcome the tendency to box up and suppress internal struggles.” As part of the campaign, the counseling center distributes “Unboxed” buttons to promote the message and offers funds for on-campus student-led mental health events.
IU also partners with U Bring Change to Mind (UBC2M), a national student-led organization that works to reduce stigmas associated with mental health care. Efforts include an annual spring event where students share anonymous stories from their mental health journeys. UBC2M student members also work with other groups, such as the Black Student Union, to create safe spaces for discussing mental health issues—including grief.
“It takes a lot of work to build trust,” Griffith says. “But it’s not uncommon for students to come back a year later, to stop in someone’s office and say, ‘I want to thank you for helping me open that door to grief and loss, and to get it out, and I’m in a better place today.’ The trauma doesn’t just, poof , go away, but by giving students a name to identify their feelings, and helping them to learn how to process them, they’re developing lifelong skills to have healthy relationships and express their emotions.”
Suicide Prevention

Research on Ways to Better Help Students
University of Oregon Eugene, Oregon
The study is unprecedented. Researchers at four universities—Duke University; the University of Nevada, Reno; the University of Oregon (UO); and Rutgers, the State University of New Jersey—are evaluating the effectiveness of four suicide intervention approaches in college and university counseling centers. It is the first multisite, National Institutes of Health (NIH)–funded, randomized controlled trial to do so—and it is fueled by a common problem: counseling centers typically don’t treat at-risk students on campus.
“Counseling centers have had to really shrink the number of services and sessions they can provide to students, and that results in referring students with longer-term issues and higher levels of need out into the community,” says Shelly Kerr, UO’s director of counseling services. “The study is designed in such a way to say, What can be done in a short amount of time? Can we do some of this work in-house rather than referring students out?”
The urgency may be rising. Fourteen percent of undergraduate and graduate students nationwide considered suicide in the 2022–23 academic year, up from 11.7 percent between 2007 and 2021, according to a study of Healthy Minds data. In addition, suicide at the high school level has become “a crisis,” says John Seeley, associate dean for research at UO and UO’s principal investigator for the NIH-funded study. In 2021, 13 percent of high school girls attempted suicide, and 30 percent had seriously considered it, according to the Centers for Disease Control and Prevention. Among LGBTQ+ teens, 22 percent attempted suicide in 2021.
The joint-university study, known as CAMPUS (the Comprehensive Adaptive Multisite Prevention of University Student Suicide), is testing four different strategies “for treating students with moderate to severe suicidal ideation through counseling centers, so that we can avoid that delay in connection to outside services,” Seeley notes. About two hundred students, aged eighteen to twenty-five, are seeking services at counseling centers across the four universities. Data collection on the success of the different treatment approaches will conclude in the fall of 2024.
Beyond the research, UO is involved in suicide prevention efforts both on and off campus. It is one of fifteen member institutions in Oregon Campuses United for Suicide Prevention, which promotes best practices, offers training, and advocates for policies and procedures to prevent suicide on Oregon campuses. The university has a suicide prevention team that provides training to faculty and staff, as well as a student suicide prevention team. UO also offers a two-day suicide first-aid education workshop for local community members.
Meeting with the counseling center’s Mental Health Access Team is the first step for students who are feeling suicidal or dealing with other mental health issues. No appointment is required. The team includes intake/crisis specialists and case managers. The university has a twenty-four-hour crisis hotline, and the number is on every student’s ID card. Anyone who is worried about a student can submit a “Report a Concern” form via the UO website. Depending on the situation, someone from the Office of the Dean of Students may contact the student and suggest on-campus resources. If the student is considered a threat to others or themselves, campus police will respond.
The study and its funding are providing an additional benefit for UO students: they are allowing the counseling center to not only provide more sessions to students at risk of suicide (normally it offers up to seven sessions per year) but place them with therapists who specialize in suicide assessment and treatment. UO is also training fourth- and fifth-year doctoral students in counseling psychology to help deliver these treatments through the Counseling Center. Five doctoral students are currently working there.
“This innovation can help meet the demand, but it also provides a preservice training opportunity,” Seeley says. “These clinicians are going to be trained in suicide-specific treatments before they go into practice.”
A Growing Epidemic
- Among college students aged 18 to 24, suicide is the second-highest cause of death.
- Suicide rates among Americans aged 10 to 24 rose by 62 percent from 2007 through 2021.
- 11 percent of adults aged 18 to 25 have had “serious thoughts” about suicide.
- 41 percent of LGBTQ+ young people age 13 to 24 seriously considered suicide in the past year.
Source: “A Growing epidemic”: Journal of College Student Psychotherapy , Centers for Disease Control and Prevention, National Alliance of Mental Illness, Trevor Project
Know the Warning Signs
- Deteriorating academic performance
- Depression, dramatic mood changes, anxiety, agitation
- Hopelessness and preoccupation with death
- Uncontrolled anger or rage
- Engagement in risky activities
- Withdrawal from friends and family
- Neglect of appearance and hygiene
- Increased alcohol use or drug use
- Giving away prized possessions
For national 24/7 help, call 988 to reach the 988 Suicide and Crisis Lifeline.
Source: Governors State University
Illustrations by Edmon de Haro
- Open access
- Published: 23 September 2024
Participant observation for inquiry-based learning: a document analysis of exam papers from an internship-course for master’s students in health services research in Germany
- Charlotte Ullrich 1 , 2 ,
- Sandra Ziegler 1 , 2 ,
- Alicia Armbruster 1 , 2 ,
- Michel Wensing 1 &
- Nadja Klafke 1 , 2
BMC Medical Education volume 24 , Article number: 1033 ( 2024 ) Cite this article
39 Accesses
Metrics details
Inquiry-based learning (IBL) is a type of problem-based learning. While IBL aims at reflecting the work of practicing researchers, only some students will pursue an academic career. We therefore designed a course that provides opportunities for IBL by applying participant observation to internship work experience inside and outside academia. Using this internship course as an example, we investigated, how master’s students in health science executed an IBL assignment regarding the application of participant observation and presentation of findings. In addition, the understanding of occupational fields provided through the IBL assignment was examined.
To determine whether learning objectives were met, a document analysis of IBL assignments comprising presentation slides and field protocols was performed. Within content analysis, a category grid was used examining (a) suitability of chosen research objectives , (b) execution of field protocols , (c) sufficiency of reporting and (d) extent of reflection .
49 IBL assignments from the years 2020–2022 were included. Sides of IBL observations were: (a) organizations providing health care ( n = 28); (b) administrations of health care ( n = 8); and (c) research institutes ( n = 13). Within students’ field protocols, the level of detail of descriptions differed. 30 assignments included reflection on the methods used and research experience. In about a third of IBL assignments, indication of observation type, theoretical background and data analysis was missing.
Using participant observation of internship work-experience for IBL can serve as a teaching tool for students to develop methodological skills. For future courses, we developed a checklist to strengthen reporting, reflection and use of theory. As internships are often integrated in degree programs in health sciences similar courses could be implemented in different programs, given qualified methodological guidance.
Peer Review reports
IBL is a type of problem-based learning in which students apply methods comparable to those of professional researchers in the respective field [ 1 ]. Across disciplines, inquiry-based learning (IBL) is considered an effective way for students to learn through self-directed investigation. Students take an active role while teachers primarily serve as facilitators rather than traditional lecturers. As a basic principle, IBL requires a learning environment that divides the scientific process into smaller units to guide students and draw their attention to specific aspects of scientific thinking. Depending on intended learning outcomes, students’ skills and interests as well as curricula requirements, formats might vary regarding suitable topics’ suitability, comprehensiveness of the learning tasks, teachers’ guidance’ and students’ autonomy (e.g. regarding provision of questions, methods and materials) [ 2 , 3 , 4 ]. In higher education, IBL has been shown to be beneficial for developing students’ inquiry skills and for improving their engagement, motivation and performance [ 5 ]. In addition, it helps students to develop skills for working in complex and unpredictable environments, enhancing critical thinking, [ 6 , 7 ]. However, despite the benefits of using IBL, it is still relatively uncommon in higher education [ 5 ].
While IBL aims at reflecting the work of practicing researchers, only some students in health-related courses will pursue an academic career. Work experience, in contrast, aims at applying academic skills to real world work settings offering students insights for the remaining studies and preparing them for the job market after graduation. Participant observation as an ethnographic method based on field work can serve as a method providing both: (a) an opportunity to apply research methods and (b) establish an in-depth understanding of occupational fields. Overall, within health sciences, the potential of participant observation is being increasingly discussed, stressing the benefits to investigate on actual practice itself, instead of indirect questionnaire or interview-accounts, [ 8 , 9 ]. In addition, ethnographic methods can contribute to narrowing the distance between theoretical knowledge and everyday practice in health service research [ 10 ]. Traditionally associated with lengthy presence and intense participation in day-to-day-life to gain holistic insights into the habits of a collective, within health sciences ethnographic data collection is often condensed to gain insights in specific sites or situations [ 11 , 12 ].
Besides general characteristics of scientific practice, learning objectives of IBL assignments based on participant observation have to address specific methodological features: Based on research literature and experience, the following learning objectives can be defined: (a) Research objectives: Participant observation is suitable for research projects seeking to understand participants’ behaviour, interactions and practices in particular situations. It requires settings where direct observations and some degree of participation are sensible. (b) Field protocols: Sound results presume field notes comprising thorough documentation with detailed accounts, separation of description and interpretation and continuing reflection. (c) Presentation of results: These aspects have to be sufficiently reported. (d) Reflection: Reflection of research experience is an inherent part of both IBL and participant observation. For these learning objectives to be met, they have to be aligned with teaching and learning activities and assessment tasks (constructive alignment) [ 13 ].
Aim and research question
Using an internship course of a masters’ program in health services research as an example, we aimed to analyze how students executed an IBL assignment with regards to the application of participant observation and presentation of findings. In addition, we aimed to examine the understanding of occupational fields provided through the IBL assignment.
Study design
Reflecting the explorative nature of the research aim, a qualitative research design was chosen comprising a document analysis of exam presentation slides and corresponding field protocols. Documents created as part of an educational process can provide empirical insights into the learning experience [ 14 ]. Our analysis is based on exam papers as anonymized aggregated data. The study aims at improving the quality of teaching and learning. With enrolment, students confirm in writing, that study data can be used for administrative and evaluative purposes. In additionethics approval for this study was granted by the Ethics Committee of the Medical Faculty of Heidelberg, Germany (S012/2016). Methods were reported according to the Checklist for the use and reporting of document analysis in health professions education research (CARDA) [ 14 ].
Data collection
All IBL assignments handed in by students after 2020 were eligible for inclusion, as the curriculum was modified in 2019. Initially collected within the study program for quality management purposes, all data were electronically filed and stored on secure servers at the Department of General Practice and Health Services Research, Heidelberg University Hospital, Germany.
Data Analysis
Data analysis focused on content using a category grid reflecting learning objectives and general internship characteristics. This deductive approach of allocating data to pre-identified themes was complemented by inductively adding sub-themes throughout data analysis. To determine whether learning objectives were met, we examined; (a) suitability of chosen research objectives in terms of observable (inter)actions, (b) execution of field protocols in terms of detail and separation of description and analysis, (c) sufficiency of presentation in terms of reporting as well as (d) extent of reflection in terms of internship and research experience. Data were analyzed by three researchers (AA, NK, CU), with prior experience in qualitative methods. Derived themes were discussed and consented regularly within the research team (AA, NK, CU, SZ). Extracted data were analyzed and reported as absolute frequencies. The software package MAXQDA, Analytics Pro 2020 was used for data management and to facilitate coding. No automation or AI tools were used.
Approach and course concept
The IBL course, which is offered each year and was first taught in 2016, was designed for a master’s degree program in health services research and implementation science at Heidelberg University, Germany. The consecutive master’s program comprises two academic years, corresponding to 120 ECTS credit points (CP), which are equivalent to 3600 h of total student workload. The goal of the master’s degree is to train students at an advanced level of health sciences including empirical research methods. A bachelor’s degree from within health science and a proof of basic skills (180 h/6 CP) in research methods are required for entering the master’s program. However, at the time of entering the program, skills in qualitative research varied and were almost exclusively limited to qualitative interviews. The masters’ program accepts 20 students per year. About 1/3 of the students are trained within a health care profession.
Aims of the course
Objectives of the course, which was designed as both an internship accompanying seminar and IBL course, were: (a) providing an opportunity to learn research skills in using (participant) observation as a qualitative research method and (b) establishing an in-depth understanding of occupational fields in health care.
Content of the course
The IBL course was taught by three teachers with a background in health services research and interdisciplinary anthropology (SZ), psychology (NK) and sociology (CU) respectively. Participant observations was introduced in a mandatory 90-minute class (SZ) highlighting its historical origin within anthropology, basic ideas of ethnography, characteristics and reach of participant observation. For writing up field notes towards field protocols, a three-column chart was recommended to distinguish observations and analysis, comprising a) a detailed description of observations, b) analytical notes , documenting the reactions, questions, interpretations and ideas of the researcher c) themes/codes derived from a first round of open coding. Prompts for fieldnotes (e.g., description of situations and participants’, communication styles) and examples for the three-column chart were provided.
Delivery format
The IBL course comprises a 7-week-long work placement accompanied by on-going monthly complementary classes. The total course credit sums up to 12 CP (360 h) including: (a) 280 h internship (b) attending four mandatory classes including the introduction, (c) assignments of keeping a field diary and documentation of three observations and (d) exam: 10–15 min oral presentation and following discussion (see Table 1 ). Students were asked to meet up with one of the teachers at least once to determine a suitable research focus. The course was designed as a pass-fail course; therefore, no mark was given.
Sample and internship characteristics
In total, 49 IBL assignments from four cohorts (defined by the year students were enrolled in the master’s program) of the years 2020–2022 were included (see Table 2 ). This corresponds to all presentations held during that time. Within two assignments field protocols were missing. Nonetheless, these could be included in the analysis, since the presentations comprised sufficient extracts of the field protocols. Variation in numbers of course participants were related to part-time students. Presentations typically included 15 slides, field protocols on average two to four pages per observation. All presentations and field protocols were in German, the main language of instruction within the master’s program. Of the students providing the presentation, five of the 49 were male and about a third had a professional background in health care, mirroring the general characteristics of the student population. Internship length was 140 to 280 h, either fulfilled over three to eight weeks full-time or part-time over a period of several months.
For the IBL assignment, most students selected internship experience ( n = 40); the remaining students ( n = 9) selected their professional employment in health care. Work places were (a) organizations providing health care ( n = 28), including nursing homes ( n = 2) and hospitals ( n = 26), of which 22 were university hospitals; (b) other organizations in health care ( n = 8), such as government departments and health insurances and (c) research institutes ( n = 13), mostly universities ( n = 8). The focus of work experiences reflected these employer types to some extent: Most students were mainly involved in research activities ( n = 31), such as literature reviews, developing questionnaires and interview guides, data analysis and overall research management. Some students ( n = 5) were involved in academic teaching, mainly in the role of (assistant) teachers. Provision of health care ( n = 4) included assisting nursing and patient involvement. Administrative tasks ( n = 8) included preparation of meetings and reports, often based on literature research.
Research objectives
A research objective was specified in all presentations, most addressed either communication in videoconferences, e.g., concerning active participation or technical difficulties ( n = 14) or some aspect of research practice ( n = 11), e.g., conducting interviews. Further objectives included patient care ( n = 7), teaching ( n = 4) and handling of Covid-19 regulations ( n = 4) (see Table 3 : section A). Observation settings were largely either virtual ( n = 20) or face-to-face meetings ( n = 23), with two observations of telephone conversation and four with mixed settings. Research participants varied and often included a mix of people: Researchers were observed most often ( n = 29), followed by health care providers ( n = 16) and patients/relatives ( n = 11). In 35 cases, observing students included themselves in the descriptions.
Field protocols
Most protocolled observations within reports included room description ( n = 45), most contained direct quotes ( n = 42), some used description of persons ( n = 12) and a few comprised sketches and/or pictures of places observed ( n = 4) (see Table 3 : section B). Overall, detail of description varied, ranging from rather abstract monosyllabic reports with little situation-specific portrayal to comprehensive, in-depth reports with lively accounts. Within all reports ( n = 49), anonymization was used, primarily employing pseudonyms for people observed. However, the degree of anonymization differed, some omitting indicating professions, gender and employment titles and some masking identifying characteristics of employers. While anonymization did not limit documenting observation within most reports, observations were reduced to mere generic enumeration of events in a few exceptional ones. For structuring field protocols all students used the suggested columns to separate observations and analytical notes ( n = 49). All but one also included the third column on emerging codes and themes. The level of detail within columns and accuracy of separation differed.
Presentation and reporting
All IBL assignments included a description of the characteristics of the employer and information on the work activities ( n = 49) (see Table 3 : section C). Most presentations ( n = 39) included literature-based background informationon communication and use of online meetings ( n = 16), challenges in health care ( n = 7), good research practice and scientific integrity ( n = 7), organization and management ( n = 5) or the impact of Covid-19 regulations ( n = 2). Some students explicitly listed theoretical concepts used ( n = 15), which were mostly communication or organizational theories.
Most ( n = 39) presentations included a description of data conduction: The majority was based on participant observation ( n = 30), often using open observation ( n = 16). Overall, methods of data analysis were sparsely reported ( n = 34): General description of data analysis without references to theoretical or methodological schools or authors ( n = 16) usually shortly indicated whether themes/codes were derived inductively and/or deductively. For describing methods of data conduction and data analysis, recommended readings of the IBL course ( n = 18) and/or the overall master’s’ course ( n = 14) were often used. 27 did not refer to methodological literature at all.
All presentations ( n = 49) included some kind of conclusion addressing results, reflections and/or recommendations. Most students discussed their observations on the content level ( n = 34) providing primarily neutral descriptions. This was discernible when students were reporting on “general conditions, settings and factors” ( n = 11) or “factors influencing virtual and face-to-face meetings” ( n = 10). Many students addressed the meaning of their findings in relation to the observed participants ( n = 19) and stated that certain communication strategies ( n = 7) or coping strategies and leadership behavior ( n = 6) could be instructive for them at future work places. Only the minority of students discussed their results on a personal level ( n = 7), and most of them valued the internship combined with the participant observation assessment as an exciting and stimulating experience ( n = 4) which made them aware of new career prospects ( n = 2). Only one student reported that she experienced the internship as a “one-sided activity” ( n = 1).
Reflection on the methods and research experience were part of most presentations ( n = 30) (see Table 3 : section D). Predominantly mentioned topics were observer roles, field access and participants’ consent. The first topic ( n = 23) included problematizations of observing while participating and the risk of overidentifying with observed people’s perspectives (“going native”) as well as observer bias due to previous experience within the field. Additionally, students saw challenges in cases where they perceived that there were too many or too few people and/or interactions accessible for observation. Field access and identification of observable situations ( n = 12) largely referred to limitations within home-office-settings and online-meetings. Reflections on informed consent ( n = 10) addressed the extent of consent, e.g., when, and how many times the student’s own role as researcher should be thematized, whom to inform, and how to handle confidentiality agreements regarding internship content. In addition, some students reflected on difficulties in determining a research focus ( n = 5).
The objective of the IBL assignment and reflection of the internship experience point to an in-depth understanding of the studied participants’ perspectives. In addressing communication and work-culture, participant observation allowed students to investigate how everyday experiences are shaped by institutional contexts. This confirms results of a study on patient shadowing as a teaching tool in premedical undergraduate education [ 17 ] and findings of a participant observations exercise within a medical students’ course on health care for refugees [ 18 ]. This highlights the potential of observations as a data collection method to understand often tacit and hidden rules that influence health care, as it is currently thematized under the term “institutional ethnography” [ 19 , 20 ].
All students embraced the IBL assignment of using participant observation taking up recommended readings and suggested strategies, e.g., the three-column chart, writing a detailed, concrete description and using direct quotes for more vividness. Students addressed significant methodological topics in ethnographic research, such as finding a focus, field access, the observer role and participants’ consent. However, reporting on some methodological aspects was incomplete: Most notably, about a third of the IBL assignments lacked indication of observation type, theoretical background and strategy of data analysis. These results show parallels to findings on reporting quality in the health sciences [ 21 , 22 ] and, in particular, difficulties regarding data analysis and relation to theory [ 23 ].
A meta-analysis of 72 studies suggested that adequate guidance to assist learners is essential to successful inquiry-based learning [ 2 ]. At the same time, there is a need to create a learning environment that allows the freedom to examine a topic independently [ 1 , 5 ]. The discussed assignment was limited to a section of the research process, focusing on formulating an initial research question, documenting three singular observations and reporting of first findings. Students were provided an introductory course, counseling and methodological prompts and references. Completed assignments and students’ feedback suggest that scope, time frame and workload of the assignment were suitable and guidance concerning field protocols sufficient. However, guidance regarding content of the presentation should be specified, highlighting reporting, reflection and the use of theoretical knowledge. Based on these noted discrepancies with recommended research practices and teaching objectives, we developed a checklist for future sources for students as a scaffold to address these topics more explicitly (see supplementary material 1 ) [ 24 ].
This study was limited to one masters’ program only; however, the diverse students’ backgrounds and skills, point to transferability of results. Data of this study were limited to written assignments, wherefore, additional aspects only presented orally were not included. From our experience, discussions in class were often more direct in addressing good scientific practice and work culture. Feedback from teachers often highlighted methodological reflections and the importance of separating normative evaluation from the description. The course was designed as a pass-fail course without specific grades. This setup could have influenced students’ performance either by allowing more freedom and self-direction or by limiting motivation and effort. Additionally, most students took the IBL course as one of the last assignments of the master’s program, often parallel to starting the master’s thesis. This, too, could have influenced motivation and performance.
Our study has shown, that the use of participant observation is not restricted to learning a scientific practice in a narrow sense. It can also provide students a better understanding of organizational culture and hierarchies of potential future work places within and beyond an academic career in health care. Participant observation is a flexible research strategy which is highly adaptable to (changing) research objectives and field settings – within IBL it is also adaptable concerning comprehensiveness of the learning task. As internships are often an inherent part of degree programs in health sciences, given qualified methodological guidance, similar courses could be implemented in other educational programs.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
Credit Points within the ECTS, 1 CP = 30h workload
European Credit Transfer and Accumulation System
- Inquiry-based learning
Pedaste M, Mäeots M, Siiman LA, de Jong T, van Riesen SAN, Kamp ET, Tsourlidaki E. Phases of inquiry-based learning: definitions and the inquiry cycle. Educational Res Rev. 2015;14:47–61. https://doi.org/10.1016/j.edurev.2015.02.003 .
Article Google Scholar
Lazonder AW, Harmsen R. Meta-analysis of Inquiry-based learning: effects of Guidance. Rev Educ Res. 2016;86(3):681–718. https://doi.org/10.3102/0034654315627366 .
Willison J. Research skill development spanning higher education: critiques, curricula and connections. J Univ Teach Learn Pract. 2018;15:2–16. https://doi.org/10.53761/1.15.4.1 .
Willison J, Peirce E, Al-Sarawi S, Donnelly F, Ricci M, Ng B. Handbook for research skill development and assessment in the curriculum. University of Adelaide; 2020.
Kori K. Inquiry-based learning in Higher Education. In: Vaz C, de Carvalho, Bauters M, editors. Technology supported active learning: student-centered approaches. Singapore: Springer Singapore; 2021. pp. 59–74.
Chapter Google Scholar
Suárez Á, Specht M, Prinsen F, Kalz M, Ternier S. A review of the types of mobile activities in mobile inquiry-based learning. Comput Educ. 2018;118:38–55. https://doi.org/10.1016/j.compedu.2017.11.004 .
Fan JY, Ye JH. The effectiveness of inquiry and practice during roject design courses at a technology university. Front Psychol. 2022;13:859164. https://doi.org/10.3389/fpsyg.2022.859164 .
Cupit C, Mackintosh N, Armstrong N. Using ethnography to study improving healthcare: reflections on the ‘ethnographic’ label. BMJ Qual Saf. 2018. https://doi.org/10.1136/bmjqs-2017-007599 .
Dixon-Woods M. What can ethnography do for quality and safety in health care? Qual Saf Health Care. 2003;12(5):326–7. https://doi.org/10.1136/qhc.12.5.326 .
Cubellis L, Schmid C, von Peter S. Ethnography in Health Services Research: Oscillation between Theory and Practice. Qual Health Res. 2021;31(11):2029–40. https://doi.org/10.1177/10497323211022312 .
Cruz EV, H. G. The use of focused ethnography in nursing research. Nurse Res. 2013;20(4):36–43.
Vindrola-Padros C, Vindrola-Padros B. Quick and dirty? A systematic review of the use of rapid ethnographies in healthcare organisation and delivery. BMJ Qual Saf. 2018;27(4):321–30.
Biggs J, Tang C, Kennedy G. Teaching for Quality Learning at University. Berkshire: Open University Press/McGraw Hill; 2023.
Google Scholar
Cleland J, MacLeod A, Ellaway RH. CARDA: guiding document analyses in health professions education research. Med Educ. 2023;57(5):406–17. https://doi.org/10.1111/medu.14964 . Epub 2022 Nov 17. PMID: 36308050.
Emerson RM, Fretz RI, Shaw LL. Writing ethnographic fieldnotes. ed.). Chicago [u.a.]: Univ. of Chicago Pr; 2011. ([2nd publ.].
Book Google Scholar
Girtler R. (2001). Methoden der Feldforschung (4., völlig neu bearb. Aufl. ed.). Wien; Köln; Weimar: Böhlau.
Wilson JW, Baer RD, Villalona S. (2019). Patient shadowing: a useful Research Method, Teaching Tool, and Approach to Student Professional Development for Premedical undergraduates. Acad Med, 94 (11).
Ziegler S, Wahedi K, Stiller M, Jahn R, Straßner C, Schwill S, Bozorgmehr K. Health and medical care for refugees: design and evaluation of a multidisciplinary clinical elective for medical students. GMS J Med Educ. 2021;38(2):Doc39. https://doi.org/10.3205/zma001435 .
Balcom S, Doucet S, Dubé A. Observation and unstitutional ethnography: helping us to see better. Qual Health Res. 2021;31(8):1534–41. https://doi.org/10.1177/10497323211015966 .
Sinding C. Using Institutional Ethnography to understand the production of Health Care disparities. Qual Health Res. 2010;20(12):1656–63. https://doi.org/10.1177/1049732310377452 .
Malterud K, Hamberg K, Reventlow S. Qualitative methods in PhD theses from general practice in Scandinavia. Scand J Prim Health Care. 2017;35(4):309–12. https://doi.org/10.1080/02813432.2017.1397257 .
Ullrich C, Stürmlinger A, Wensing M, Krug K. Qualitative research methods in medical dissertations: an observational methodological study on prevalence and reporting quality of dissertation abstracts in a German university. BMC Med Res Methodol. 2020;20(1):301.
Wright MC. Making sense of data: how Public Health Graduate Students Build Theory through qualitative research techniques. Qual Health Res. 2007;17(1):94–101. https://doi.org/10.1177/1049732306294296 .
O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–51. https://doi.org/10.1097/acm.0000000000000388 .
Download references
Acknowledgements
The authors would like to thank Lara Cordes (LC) for contribution to a first draft for data extraction themes in an early phase of the study.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and affiliations.
Medical Faculty, Heidelberg University, Heidelberg, Germany
Charlotte Ullrich, Sandra Ziegler, Alicia Armbruster, Michel Wensing & Nadja Klafke
Department of General Practice and Health Services Research, Heidelberg University Hospital, Im Neuenheimer Feld 130.3, 69120, Heidelberg, Germany
Charlotte Ullrich, Sandra Ziegler, Alicia Armbruster & Nadja Klafke
You can also search for this author in PubMed Google Scholar
Contributions
NK and CU drafted and prepared the manuscript, AA, MW and SZ provided substantial comments at different stages of the manuscript. MW is the head, CU the coordinator of the master’s program in health services research and implementation science at Heidelberg University, Germany. NK, CU and SZ jointly teach the IBL-course within this program, with SZ teaching the introductory class on ethnographic methods. All three designed this study. AA, LC, NK, CU and SZ collaborated on planning the data analysis. AA supported data management. AA, NK, and CU reviewed, extracted and analyzed the data. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Charlotte Ullrich .
Ethics declarations
Ethical approval and consent to participate.
Approval for the study was obtained from the Ethics Committee of the Medical Faculty of Heidelberg University Hospital, Germany (S012/2016). With enrolment, students confirm informed in writing that study data can be used for administrative and evaluative purposes. As this study aims at improving quality of teaching and is based on exam papers, a waiver for additional informed consent was granted. Any information with the potential to identify individuals has been anonymized.
Disclaimers
There are no conflicts of interest to disclose.
Previous presentations
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Ullrich, C., Ziegler, S., Armbruster, A. et al. Participant observation for inquiry-based learning: a document analysis of exam papers from an internship-course for master’s students in health services research in Germany. BMC Med Educ 24 , 1033 (2024). https://doi.org/10.1186/s12909-024-05740-4
Download citation
Received : 07 August 2023
Accepted : 02 July 2024
Published : 23 September 2024
DOI : https://doi.org/10.1186/s12909-024-05740-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Document analysis
- Participant observation
- Qualitative methods
- Master’s degree program
- Medical education and evaluation
BMC Medical Education
ISSN: 1472-6920
- General enquiries: [email protected]
- Fact sheets
- Facts in pictures
- Publications
- Questions and answers
- Tools and toolkits
- Endometriosis
- Excessive heat
- Mental disorders
- Polycystic ovary syndrome
- All countries
- Eastern Mediterranean
- South-East Asia
- Western Pacific
- Data by country
- Country presence
- Country strengthening
- Country cooperation strategies
- News releases
- Feature stories
- Press conferences
- Commentaries
- Photo library
- Afghanistan
- Cholera
- Coronavirus disease (COVID-19)
- Greater Horn of Africa
- Israel and occupied Palestinian territory
- Disease Outbreak News
- Situation reports
- Weekly Epidemiological Record
- Surveillance
- Health emergency appeal
- International Health Regulations
- Independent Oversight and Advisory Committee
- Classifications
- Data collections
- Global Health Observatory
- Global Health Estimates
- Mortality Database
- Sustainable Development Goals
- Health Inequality Monitor
- Global Progress
- World Health Statistics
- Partnerships
- Committees and advisory groups
- Collaborating centres
- Technical teams
- Organizational structure
- Initiatives
- General Programme of Work
- WHO Academy
- Investment in WHO
- WHO Foundation
- External audit
- Financial statements
- Internal audit and investigations
- Programme Budget
- Results reports
- Governing bodies
- World Health Assembly
- Executive Board
- Member States Portal
World Innovation Summit for Health (WISH) 2024: ‘Humanizing Health: Conflict, Equity and Resilience’
The World Innovation Summit for Health (WISH), an initiative of Qatar Foundation for Education, Science and Community Development, will take place from 13–14 November 2024 in Doha, Qatar. WISH is a global healthcare community dedicated to capturing and disseminating the best evidence-based ideas and practices.
In December 2023, following discussions between Her Highness Sheikha Moza bint Nasser, Chairperson of Qatar Foundation and WHO Director-General Tedros Ghebreyesus, WISH and WHO established a strategic partnership , formalising a longstanding relationship between the two organizations, building on a track record of impact and reflecting joint resolve to focus attention on solving pressing global health challenges.
Over two days, more than 2,000 health policy makers, innovators, entrepreneurs, researchers and practitioners will convene at the Qatar National Convention Centre to look for innovative solutions to some of the world’s biggest health challenges. The theme of this year’s summit is ‘Humanizing Health: Conflict, Equity and Resilience’ and will highlight the need for progress in health to support everyone, leaving nobody behind and building resilience, especially among vulnerable societies and in areas of armed conflict.
WISH and WHO are collaborating to create a series of evidence-based reports and policy papers that will be released at WISH. The reports aim to provide policy recommendations for innovative, practical solutions to strengthen people-centred health systems that can provide equitable, accessible and quality health for all individuals, families and their communities. The WHO-led reports, featured within plenary sessions, focus on elimination of tuberculosis, the growing importance of palliative care, and protecting health in armed conflict.
Reflecting the importance of translating research into practical solutions, additional sessions will be structured around WHO-led policy papers on community engagement and indigenous health, women’s cancers in the Eastern Mediterranean Region, and women in the health and care workforce in the Eastern Mediterranean Region.
Within the overall theme, November’s global gathering will feature four ‘tracks’, categorizing sessions into sub-themes:
- Health and armed conflict, covering pain management, disability, hunger and mental health
- Health of vulnerable and minority populations, considering TB in refugees and migrants and palliative care
- System level innovation and change, such as antimicrobial resistance and the ethics of AI in health
- Community-led engagement and interventions, including obesity and women’s cancers in the region
The biennial meeting will feature more than 200 experts in health speaking about evidence-based ideas and practices in healthcare innovation to address the world’s most urgent global health challenges.
- Health Workforce
- Our duty of care : a global call to action to protect the mental health of health workers
- Global Health and Care Worker Compact
- Tuberculosis
- Antimicrobial resistance
- Projects and Investigations
- Nation / World
- Entertainment
- Newsletters
- Give Feedback
- Connect With Us
- For Subscribers
- Staff Directory
- Contributor Content
Opinion: Eric Hovde: Address root causes of gun violence. Don't restrict law-abiding citizens
Cities across america with the strictest gun laws, like new york, dc, and chicago, have some of the highest violent crime rates. adding more restrictions would be wrong and dangerous..

Editor's Note: The Ideas Lab asked the Democrat and Republican candidates for the U.S. Senate to submit 1,000 word essays on how they would tackle gun violence, the issue Wisconsinites surveyed as part of the Main Street Agenda project said is the second most significant problem they face heading into the Nov. 5 election.
Sadly, today, a multitude of underlying issues have resulted in tragic acts of violence and firearms are among those instruments used to carry out these incidents.
While Sen. Tammy Baldwin argues for further restrictions on law-abiding citizens, real progress to prevent acts of violence carried out with a firearm, or any other mechanism, requires addressing the underlying problems. We need to focus on solutions such as enhancing mental health resources, effectively enforcing existing laws , and improving school safety.
60% of perpetrators of mass shootings have mental health issues
Our nation is facing a mental health crisis. Too often, individuals growing up without a strong support system face mental health problems and are turning to acts of violence.
This has tragically been displayed in the increase of mass shootings in America and must be addressed. Especially those that affect our most vulnerable population, our children. As a grandfather of three, I take this issue very seriously and in Washington will promote policies to keep our children safe.
Tammy Baldwin: Common sense firearm safety laws can curb gun violence epidemic
A study found 60% of perpetrators of mass shootings in the United States displayed symptoms of a mental health disease including depression and paranoia. We must provide schools with the tools needed to address this growing crisis.
The mental health crisis not only leads to tragic mass shootings, but is a major factor in the leading cause of death in gun violence which is suicide. For every 100 gun deaths in Wisconsin, 71 are suicides. That is heartbreaking.
Nearly 60% of Wisconsin high school students feel anxious, depressed or suicidal. Too often politicians are focused on reactive policies and fail to promote proactive solutions. I believe we should improve access to mental health care for those at-risk and their families to prevent tragedies and create an environment of hope.
When it comes to ensuring individuals showing signs of self-harm or violence don’t have access to a firearm, a due process method is extremely important, but it is critical that any measure taken respects the constitutional rights of law-abiding citizens.
It is also critical that we work to enhance our school’s physical security and improve their preparedness.
Federal education funds should be directed to school security, safety
I would take steps to redirect federal education funds towards bolstering school security by strengthening points of entry, allowing staff to better track and verify visitors.
We also need to put school resource officers back in schools to foster an environment of safety and facilitate a quick response to any incident. School resource officers would be able to provide training to staff and students, ensuring emergency drills are thorough and effective.
Throughout this process, we must engage parents and community leaders in each school by involving them in the implementation of safety procedures while building partnerships with local law enforcement.
Social media, video games play a role in gun violence affecting youth
Our nation has promoted a culture of violence in which children are saturated in hyper- violent video games and social media platforms that fuel further acts of aggression in our communities, specifically those already struggling from gang activity and gun- related crimes.
Both police and violence prevention workers have cited social media as a challenge in curbing gun violence.
I strongly support the bipartisan Kids O ff Social Media Act which would set a minimum age of 13 to use social media platforms and stop social media companies from promoting algorithmically-targeted content to their users under the age of 17. Getting our children away from the toxic and violent culture promoted on social media and engaging them with community leaders and support systems while promoting strong familial values can play an important role in reducing violence impacting children and teens.
Fully fund the police and enforce existing gun laws
It is also critical that we fully fund and support law enforcement so they can protect our children and our streets effectively. Over the past decade-and-a-half, the total number of law enforcement officers in Wisconsin has dropped 11% to a new record low in the state. This dangerous trend needs to change and it starts by giving our police the tools needed to be successful.
I also strongly support enforcing existing gun laws that are focused on keeping guns out of the hands of criminals. This can be done by improving data sharing and collaboration between law enforcement agencies investigating gun-related crimes, cracking down on gang violence while prosecuting to the fullest extent of the law illegal possession and trafficking of firearms, and properly funding technology such as forensic tools to track down guns used in crimes.
Baldwin’s push for further restrictions on law-abiding citizens does not work for one simple reason: criminals don’t obey the law.
Opinion: Are we 'Ready For It?' Taylor Swift endorsement causes voter registration surge.
We know that cities across America with the strictest gun laws, like New York, DC, and Chicago, have some of the highest violent crime rates. The vast majority of criminals get their hands on firearms through illegal means. Therefore, adding more restrictions on law-abiding citizens and infringing upon their rights would be not only wrong but dangerous.
Some of America and Wisconsin’s worst acts of violence were carried out without firearms, highlighting the importance of tackling the root causes of what is motivating individuals to commit horrible crimes. Tragically, in Waukesha a deranged man drove an SUV through the annual Christmas parade, killing 6 Wisconsinites and injuring 62 others. But we are not talking about banning SUVs because they were used as an instrument to carry out an act of violence. We need to get serious about addressing the underlying issues leading to violence.
Owning a firearm is the right of every law-abiding citizen which was established by our Founding Fathers in the Second Amendment. Individual rights are at the core of the great American experiment and the right to bear arms ensures Americans have the means to defend themselves and their loved ones against tyranny, oppression, and any danger.
Protecting individual rights while addressing the issue of gun violence requires a balanced approach. To protect our children and make our state and nation safer, we must focus on proactive measures that address the root causes rather than imposing restrictions on law-abiding citizens. By fostering commonsense efforts that engage communities, parents, and law enforcement we can take meaningful steps forward, building a safer future while upholding the liberties that define America.
Eric Hovde is the Republican candidate for the U.S. Senate in Wisconsin. He is the CEO of Hovde Properties , a Madison-based real estate development company.
Respondents in a 'WisconSays' survey by the UW-Survey Center ranked gun violence as the second most significant problem facing Wisconsin. Gun violence is a broad issue with complex roots. There are four aspects we’d like you to touch on in your submission:1. Firearms are the leading cause of death for children and teens In America. What would you propose to reverse this disturbing reality?2. As of 10 a.m. on September 5, there have been 30 mass killings in the U.S. this year. What legislation would you support to curb mass shootings?3. Violence at schools is a contributor to the statistics behind both mass killings and youth death causes. On Sept. 4, two teachers and two students were killed at a Georgia high school, and nine students were injured. A 14-year-old student and his father have been charged in connection with their deaths. What more can be done to prevent such tragedies from reoccurring?4. Death by suicide is a significant factor in gun violence. Firearms are the most common means of suicide. On average, for every 100 gun deaths in Wisconsin, 71 are suicides. What can be done to prevent such tragedies? Do you support red flag laws or similar measures that establish a process for judges to remove firearms from individuals with mental health conditions?
Vladivostok City
| Overview | Map | Directions | Satellite | Photo Map |
| Overview | Map | Directions |
| Satellite | Photo Map |
| Tap on the map to travel |
Notable Places in the Area
Soviet submarine s-56.

Zolotoy Bridge

Dynamo Stadium

Locales in the Area
Vladivostok.

- Location: Primorsky Krai , Russian Far East , Russia , Eastern Europe , Europe
- View on OpenStreetMap
Vladivostok City Satellite Map
- Churkino Locality
- Kanal Suburb, 5 km south
- Pospelovo Suburb, 5 km south
- Terebilovka Locality, 7 km southeast
- Uliss Locality, 7 km east
Landmarks in the Area
- Poluostrov Shkota Peninsula
- Bukhta Fëdorova Bay
- Tranzitnaya Gavan’ Harbour
- Mys Kupera Cape
- Cape Burnyy Cape
Popular Destinations in Primorsky Krai
Curious places to discover.
- About our Authors
- SRAS: Study Abroad or Online
- Folkways: Folk Culture
- PopKult: Popular Culture
- Students Abroad: Travel Guides
- Museum Studies Abroad: High Culture and City Planning

Vladivostok: A Short History of Russian Rule in the East

Primorsky Krai, where Vladivostok is located (near the southern tip).
The construction of Vladivostok was the culmination of Russia’s long drive to establish a major naval presence in the Pacific Ocean and help solidify its hold on the eastern portion of its empire. The land it the city is built on was previously claimed (but, many say, never effectively ruled) by China. It was sparsely populated by Chinese and indigenous peoples when the region was transferred to Russia via the Treaty of Aigun from the Chinese Qing Empire in 1858 at Russia’s request. Russia had already moved troops and settlers into the region and the Qing Empire, then relatively weak, felt it had little choice in ceding the territory

The area also had obvious value as a diplomatic and economic outpost – lying just a short boat ride from Japan, China, and the Korean peninsula.
In 1871, Russia’s Pacific Fleet (then known as the Siberian Military Flotilla) was moved to Vladivostok from Nikolayevsk-on-Amur and bolstered with several ships sent from the Baltic Fleet (based in St. Petersburg). At the same time, the commercial port was also moved from Nikolayevsk-on-Amur, giving a boost to the economy. In 1903, the Trans-Siberian Railway connected to the city, opening it to the valuable markets located in the west.
A woman strolls the hilly streets of Vladivostok. Photo by former SRAS student Joshua Blackwelder.
By the time the Russo-Japanese War started in 1904, the city was a major part of the Russian empire. Several theatres had been opened, newspapers were being published, and an institution of higher education, the Oriental Institute, had been founded. There were hundreds of buildings lining lighted streets, interspersed with parks and trees.
Vladivostok suffered heavy losses in that war, but recovered relatively quickly. Afterwards, despite revolts by local sailors in 1906, it would continue to grow until the Revolution began in 1917. As WWI was still raging, American, British, and Japanese forces occupied the city together with White Army troops in order to protect supplies, supply lines, and the British and Japanese citizens still resident in the city. The armies collectively resisted the Red Army during the Russian Civil War. The fall of Vladivostok in 1922, after the end of WWI and the departure of the foreign troops, is often cited as one of the final events of the Civil War, sealing the Bolshevik victory.
Under the Soviets, growth and development continued with industrial, military, communication, and transportation infrastructure all being built. The region around the city would also be home to several gulags to house political prisoners and POWs in WWII and the Korean War (including several American and Chinese pilots who served in the later). Vladivostok was declared a “closed” city in 1958 – meaning that those visiting the city (even Soviet citizens) had to obtain special permission to enter. Vladivostok “reopened” in 1991.
Today, the city of Vladivostok has an official population of about 600,000, consisting mostly of ethnic Russians, with small minorities of Chinese, Koreans, Japanese, and indigenous peoples. However, there are a great number of illegal Chinese immigrants in the city, which staff the city’s most popular markets and restaurants. While the total number of Chinese there is not exactly known, many estimates put the number at around 10,000 and the influences of Chinese culture in the city’s daily life can be easily felt.
One of only four major seaports serving a gigantic country, Vladivostok has become a major commercial hub – mainly for goods brought from China, Japan, and Korea, and through both legal and illegal means.
Take one of the city’s best known industries: the importation of automobiles. Many of Vladivostok’s early car importers got their starts by essentially pirating ships loaded with Japanese cars that arrived to the then relatively ill-guarded and corrupt port. In a National Geographic article published this July entitled “Road Tripping the Trans-Siberian,” two reporters tell of meeting such men. According to their stories, the process was simple: hold up a boat with some guns and some friends, steal one of the cars, sell it, and use the proceeds to continue to buy and sell cars.
Car importing remains a big business (and is now much better regulated, although the city retains a reputation for corruption). In parking lots around the port, one can always find “ peregonshikii .” This is the Russian term for those who work driving cars over the still largely unpaved and ill-kept highway that links Vladivostok to the booming car markets in western Russia. The cars are driven individually rather than in larger transport trucks.
Auto importation is, of course, not the city’s only industry. Other major industries center largely on the port: fishing, shipping, and ship building and repair – including maintenance of the naval fleet which is still based there.
Over the last few years, the city’s troubled mayoral office has been the source of unpleasant headlines. In 2004, shortly after losing his reelection bid, former mayor Yuri Kopylov was arraigned on charges of “abuse of office” for handing a construction contract to a company without accepting other tenders. He was given a four-year suspended sentence. His successor, Vladimir Nikolaev, was also put on trial in 2007 and removed from office on charges that he had illegally paid for security services with municipal funds. Seeing two mayors on trial in just a few years, voter participation in mayoral campaigns has sunk by 50% since the start of the decade.
Environmental issues are also a concern for the city. While the city proper is slightly better off, two-thirds of Vladivostok’s suburbs are categorized as too polluted to be lived in. Local geographic conditions compound the problem, with high hills preventing winds from sweeping out the air pollution. According to investigative reporting from the International Herald Tribune, funds intended to address the environmental issues get siphoned off, and only 1% funds that come from fines on polluters are used for their intended purpose: fighting pollution.
The city has also recently been the focus of investment, including new construction and renovations. It has made itself more hospitable to business people and tourists – and several English-speaking, luxury hotels have sprung up. The local train station and the airport have both been refurbished. Several foreign companies now have a presence there. However, nearly all complain that heavy bureaucracy and crumbling infrastructure (in everything from transport to logistics to communications) are holding back Vladivostok from its full potential as an economic hub. Also, according to government estimates, (in perhaps what should be seen as a conservative estimate), 25% of the population lives below the poverty line. With that statistic, retail and service sectors are also obviously held back.
A US naval ship and sailors in Vladivostok.
Despite its problems, Vladivostok’s residents are often proud to be part of the “Eastern Ruler” of Russia. With its steep hills looking down on ships and ports, and streets dotted with Chinese and Korean shops and restaurants, the city is often compared to San Francisco in its look and feel.
The city also hosts nine universities. Far Eastern National University (FENU), based in Vladivostok, is one of Russia’s five largest institutions with 40,000 plus students. It was also ranked thirteenth in the last ranking of top universities in Russia by Russia’s Ministry of Education. FENU will soon become the basis of a new “Far Eastern Federal University,” meaning more federal funds, the construction of new facilities (particularly for the sciences), and the ability to absorb other universities (such as Khabarovsk State, which has already become the Far Eastern National University for the Humanities).
Adding to the city’s eclectic culture, the United States Navy also holds a regular presence there and regularly provides sailors with shore-time there. The Navy also often hosts goodwill events in Vladivostok – everything from Fourth of July celebrations to sandwich-making competitions (as was held in early 2008).
Students have mentioned that other points of interest include exploring the port’s submarine museums, visiting the historic train station, trying the excellent local Chinese food and just strolling the hilly city streets. Visiting the taiga that lies just above the city is also popular for tourists, as the forest is home to tigers and other exotic and endangered species.
Like many cities today, Vladivostok battles pollution, depleting resources, corruption, and poverty. But its strategic location and its proximity to East Asian countries makes it a vital outpost for Russia and an extremely interesting experience for students and tourists.
Learn More about Programs in Vladivostok!
Experience the Russian Far East with SRAS
About the Author

Josh Wilson
Josh has been with SRAS since 2003. He holds an M.A. in Theatre and a B.A. in History from Idaho State University, where his masters thesis was written on the political economy of Soviet-era censorship organs affecting the stage. He lived in Moscow from 2003-2022, where he ran Moscow operations for SRAS. At SRAS, Josh still assists in program development and leads our internship programs . He is also the editor-in-chief for the SRAS newsletter , the SRAS Family of Sites , and Vestnik . He has previously served as Communications Director to Bellerage Alinga and has served as a consultant or translator to several businesses and organizations with interests in Russia.
Program attended: All Programs
View all posts by: Josh Wilson
Primorsky Krai
- Interim Governor of the Primorsky Krai: Tarasenko Andrei Vladimirovich
- Chairman of the Primorsky Krai Legislative Assembly: Rolik Alexander Ivanovich
- Capital of the Region, thousand persons: Vladivostok - 606.6 (on the 1st of Jan. 2017)
- The Distance to Moscow, km: 9,302
- Urban Population, %: 77.21 (2017)
- Population, thousand persons: 1,913 (on the 1st of Jan. 2018)
- Population Density, persons per sq. km: 11.62 (on the 1st of Jan. 2018)
- Area, thousand sq. km: 165 (on the 1st of Jan. 2018)
- First Person Official Web-Site
- Statistics Agency Official Web-Site
- Old and Failing Housing Stock, %: 2.00 (2016)
- Number of Employed per One Retired Person: 1.82 (2014)
- Per Capita Monthly Income, Rubles: 33,259.50 (2017)
- GRP per Capita, rubles: 382,587 (2016)
- GRP, billion rubles: 737 (2016)
- Gini Index: 0.39 (2017)
- Key Indicators
Agriculture
Demographics, electricity, environment, fixed assets, foreign trade, gross regional product, household income and consumption, industrial production, investment and construction, living conditions, population projections, services to households.
- Natural population increase
- Population density
- Urban population share
- Crude birth rate
- Crude death rate
- Fertility rate
- Life expectancy at birth
- Net migration
- Population forecast
- Young population forecast
- Employable age population forecast
- Retirement age population forecast
- Life expectancy at birth forecast
- Net migration forecast
- Labor force
- Employed population
- Unemployed population
- Labor force participation rate
- Unemployment rate
- Employment rate
- Personal income per capita
- Personal consumption expenditure per capita
- Poverty rate
- Life expectancy
- Female life expectancy at birth
- Male life expectancy
- Infant mortality rate
- Number of beds
- Crimes registered
- Offenders identified
- Particularly serious crimes
- Serious crimes
- Minor offenses
- Economic crimes
- Terrorist offenses
- Extremist crimes
- Drug trafficking
- Arms trafficking
- Murder and attempted murder
- Acceptance of bribe
- Giving a bribe
- Children in preschool education
- Students in secondary professional education
- Students in tertiary education
- Specialists completed tertiary education
- Postgraduate students
- Doctoral students
- Volume of total services
- Volume index of total services
- Value of consumer services
- Value of housing services
- Value of transport services
- Value of medical services
- GRP per capita
- GRP per capita growth
- Retail trade volume growth
- Industrial production index
- Industrial production index YoY
- Stock of fixed assets
- New fixed capital stock created
- Depreciation of fixed assets
- Deterioration rate of fixed assets
- Minimum grocery basket inflation
- Food goods inflation
- Non-food Inflation
- Services Inflation
- Fixed capital investment value
- Fixed capital investment growth rate
- New residential dwellings
- Electricity production
- Electricity consumption
- Electricity exports abroad
- Monthly electricity production
- Arable land
- Arable land share
- Forest area share
- Emissions of air pollutants
- Volume of emissions of air pollutants
- Neutralized pollutants
- Personal cars
- Number of cell phones
- Number of personal computers
- Size of dwellings
- Average product consumption per day
- Dwellings equipped with piped water
- Agricultural production
- Livestock production
- Crop production
- Livestock and poultry weight gain
- Grains and legumes
- Standing wood burned
- Terms of Use
- Privacy Policy
Our Privacy Statement & Cookie Policy
Okay to continue Our website uses cookies to improve your online experience. They were placed on your computer when you launched this website. You can change your personal cookie settings through your internet browser settings.
IMAGES
VIDEO
COMMENTS
500 Words Essay on Health Education. We all know that health education has become very important nowadays. It refers to a career where people are taught about healthcare. Professionals teach people how to maintain and restore their health. In other words, health does not merely refer to physical but also mental, social and sexual health.
URGENT NEED FOR NEW DIRECTIONS IN EDUCATION-HEALTH RESEARCH. Americans have worse health than people in other high-income countries, and have been falling further behind in recent decades ().This is partially due to the large health inequalities and poor health of adults with low education ().Understanding the health benefits of education is thus integral to reducing health disparities and ...
This essay about the interplay between health and education discusses how health education acts as a vital component in human development. It highlights the role of health education in empowering individuals and communities to make informed health choices, emphasizing its impact on both physical and mental well-being.
A clear understanding of the macro-level contexts in which education impacts health is integral to improving national health administration and policy. In this research, we use a visual analytic approach to explore the association between education and health over a 20-year period for countries around the world. Using empirical data from the OECD and the World Bank for 26 OECD countries for ...
This paper strives to present current evidence and examples of how the collaboration between health education and health literacy disciplines can strengthen K-12 education, promote improved health, and foster dialogue among school officials, public health officials, teachers, parents, students, and other stakeholders.
Essay on Health Education: Health issues are constant in human life. But we can educate ourselves to improve our health condition and standard of living. Thus, health education is gaining importance. Especially in developed countries, health should be given maximum focus because people are unaware of basic hygiene principles. Moreover, in the ...
Supporting Abortion: Empowering Women's Rights and Health. The issue of abortion is a topic that invokes a range of emotions and opinions. In this essay, we will delve into the reasons for supporting abortion, emphasizing the importance of women's rights, bodily autonomy, and the advancement of public health.
They teach students about nutrition, physical education, and hygiene. Schools also organize health camps and invite doctors to talk about different health topics. Conclusion. Health awareness is a key to a healthy life. It helps us make wise choices, prevent diseases, and lead a happy, healthy life. ... 500 Words Essay on Health Awareness What ...
Short Essay On Health Education. Health education is a crucial aspect of overall health and wellness, as it plays a vital role in helping individuals make informed decisions about their health and well-being. Health education can encompass a range of topics, including personal health, nutrition, physical activity, disease prevention, and ...
DOI 10.3386/w12352. Issue Date July 2006. There is a large and persistent association between education and health. In this paper, we review what is known about this link. We first document the facts about the relationship between education and health. The education 'gradient' is found for both health behaviors and health status, though the ...
Sample Essay On Health in 300 Words. Health is undeniably one of the most precious aspects of life. It encompasses not only the absence of diseases but also the presence of physical, mental, and emotional well-being. In this essay, we will explore the multifaceted importance of health in our lives. Firstly, physical health is the cornerstone of ...
At UNESCO, inclusive and transformative education starts with healthy, happy and safe learners. Because children and young people who receive a good quality education are more likely to be healthy, and likewise those who are healthy are better able to learn and complete their education. Guided by the UNESCO Strategy on education for health and ...
Education and health and wellbeing are intrinsically linked. The evidence behind the importance of education as a determinant of health is amongst the most compelling. Education is strongly associated with life expectancy, morbidity, health behaviours, and educational attainment plays an important role in health by shaping opportunities, employment, and income.
1. Education and Advocacy: Advanced practice nurses play a crucial role in educating individuals, families, and communities about health promotion, disease prevention, and self-care practices. They provide evidence-based information and resources to empower individuals to make informed decisions about their health. 2.
500+ Words Essay on Health. Essay on Health: Health was earlier said to be the ability of the body functioning well. However, as time evolved, the definition of health also evolved. It cannot be stressed enough that health is the primary thing after which everything else follows. When you maintain good health, everything else falls into place.
It is now widely recognized that health outcomes are deeply influenced by a variety of social factors outside of health care. The dramatic differences in morbidity, mortality, and risk factors that researchers have documented within and between countries are patterned after classic social determinants of health, such as education and income (Link and Phelan, 1995; CSDH, 2008), as well as ...
February 12, 2024 by Prasanna. Essay on Health: The World Health Organization defines health as a state of mental, physical, and social well-being, and not merely physical well-being. Individuals who are healthy in mind are automatically healthy in their bodies. Good health is man's greatest possession. A healthy person is one who can ...
Health Education Journal is a peer reviewed journal publishing high quality papers on health education as it relates to individuals, populations, groups and communities vulnerable to and/or at risk of health issues and problems. A strongly educational perspective is adopted with a focus on activities, interventions and programmes that work well in the contexts in which they are applied.
Health Education Essay 1 (200 Words) In a lay man's term, Health Education is defined as a program which teaches an individual or a community about the methods to improve their health conditions by providing health literacy. Health Education covers various aspects, ranging from social health, mental health to sexual and reproductive health.
UO also offers a two-day suicide first-aid education workshop for local community members. Meeting with the counseling center's Mental Health Access Team is the first step for students who are feeling suicidal or dealing with other mental health issues. No appointment is required. The team includes intake/crisis specialists and case managers.
Inquiry-based learning (IBL) is a type of problem-based learning. While IBL aims at reflecting the work of practicing researchers, only some students will pursue an academic career. We therefore designed a course that provides opportunities for IBL by applying participant observation to internship work experience inside and outside academia. Using this internship course as an example, we ...
The World Innovation Summit for Health (WISH), an initiative of Qatar Foundation for Education, Science and Community Development, will take place from 13-14 November 2024 in Doha, Qatar. WISH is a global healthcare community dedicated to capturing and disseminating the best evidence-based ideas and practices.In December 2023, following discussions between Her Highness Sheikha Moza bint ...
The mental health crisis not only leads to tragic mass shootings, but is a major factor in the leading cause of death in gun violence which is suicide. For every 100 gun deaths in Wisconsin, 71 ...
Vladivostok City. Location: Primorsky Krai, Russian Far East, Russia, Eastern Europe, Europe. View on OpenStreetMap. Latitude. 43.104° or 43° 6' 14" north. Longitude. 131.8694° or 131° 52' 10" east. Elevation. 5 metres (16 feet)
By the time the Russo-Japanese War started in 1904, the city was a major part of the Russian empire. Several theatres had been opened, newspapers were being published, and an institution of higher education, the Oriental Institute, had been founded. There were hundreds of buildings lining lighted streets, interspersed with parks and trees.
Artyom Lukin, Deputy Director for Research, School of Regional and International Studies, Far Eastern Federal University in Vladivostok, explains that during the First Opium War that occurred between September 1839 and August 1842, fought between Britain and the Qing Dynasty, the former began exploring and mapping this stretch of the coast.
Interim Governor of the Primorsky Krai: Tarasenko Andrei Vladimirovich Chairman of the Primorsky Krai Legislative Assembly: Rolik Alexander Ivanovich Capital of the Region, thousand persons: Vladivostok - 606.6 (on the 1st of Jan. 2017) The Distance to Moscow, km: 9,302 Urban Population, %: 77.21 (2017) Population, thousand persons: 1,913 (on the 1st of Jan. 2018)