

Pathways of Addiction: Opportunities in Drug Abuse Research (1996)
Chapter: 1. introduction, 1 introduction.
Drug abuse research became a subject of sustained scientific interest by a small number of investigators in the late nineteenth and early twentieth centuries. Despite their creative efforts to understand drug abuse in terms of general advances in biomedical science, the medical literature of the early twentieth century is littered with now-discarded theories of drug dependence, such as autointoxication and antibody toxins, and with failed approaches to treatment. Eventually, escalating social concern about the use of addictive drugs and the emergence of the biobehavioral sciences during the post-World War II era led to a substantial investment in drug abuse research by the federal government (see Appendix B ). That investment has yielded substantial advances in scientific understanding about all facets of drug abuse and has also resulted in important discoveries in basic neurobiology, psychiatry, pain research, and other related fields of inquiry. In light of how little was understood about drug abuse such a short time ago, the advances of the past 25 years represent a remarkable scientific accomplishment. Yet there remains a disconnect between what is now known scientifically about drug abuse and addiction, the public's understanding of and beliefs about abuse and addiction, and the extent to which what is known is actually applied in public health settings.
During its brief history, drug abuse research has been supported mainly by the federal government, with occasional investments by major private foundations. At the federal level, the lead agency for drug abuse research is the National Institute on Drug Abuse (NIDA), which supports
85 percent of the world's research on drug abuse and addiction. Other sponsoring agencies include the National Institute of Mental Health (NIMH), the National Institute on Alcohol Abuse and Alcoholism (NIAAA), and the Substance Abuse and Mental Health Services Administration (SAMHSA), all in the Department of Health and Human Services; as well as the Office of Justice Programs (OJP) in the Department of Justice. Throughout the federal government, the FY 1995 investment in drug abuse research and development was $542.2 million, which represents 4 percent of the $13.3 billion spent by the federal government on drug abuse (ONDCP, 1996). By comparison, $8.5 billion (64 percent of the FY 1995 budget) was spent on criminal justice programs, 1 $2.7 billion (20 percent) on treatment of drug abuse, and $1.6 billion (12 percent) on prevention efforts.
In 1992, the General Accounting Office (GAO) released a report Drug Abuse Research: Federal Funding and Future Needs, which recommended that Congress review the place of research in drug control policy and its modest 4 percent share of the drug control budget. The report questioned whether the federal commitment to research was adequate, given the enormity of research needs (GAO, 1992), and whether adequate evaluation research was being conducted to determine the efficacy of various drug control programs. In FY 1995, drug abuse research was still little more than 4 percent of the entire drug control budget.
In January 1995, NIDA requested the Institute of Medicine (IOM) to examine accomplishments in drug abuse research and provide guidance for future research opportunities. This report by the IOM Committee on Opportunities in Drug Abuse Research focuses broadly on opportunities and priorities for future scientific research in drug abuse. After a brief review of major accomplishments in drug abuse research, the remainder of this chapter discusses the vocabulary and basic concepts used in the report, highlights the importance of the nation's investment in drug abuse research, and explores some of the factors that could improve the yield from that investment.
MAJOR ACHIEVEMENTS IN DRUG ABUSE RESEARCH
There have been remarkable achievements in drug abuse research over the past quarter of a century as researchers have learned more about the biological and psychosocial aspects of drug use, abuse, and dependence. Behavioral researchers have developed animal and human mod-
|
| Criminal justice programs include interdiction, investigation, international efforts, prosecution, correction efforts, and intelligence programs. |
els of drug-seeking behavior, that have, for example, yielded objective measures of initiation and repeated administration of drugs, thereby providing the scientific foundation for assessments of "abuse liability" (i.e., the potential for abuse) of specific drugs (see Chapter 2 ). This information is an essential predicate for informed regulatory decisions under the Food, Drug and Cosmetic Act and the Controlled Substances Act. Taking advantage of technological advances in molecular biology, neuroscientists have identified receptors or receptor types in the brain for opioids, cocaine, benzodiazepines, and marijuana and have described the ways in which the brain adapts to, and changes after, exposure to drugs. Those alterations, which may persist long after the termination of drug use, appear to involve changes in gene expression. They may explain enhanced susceptibility to future drug exposure, thereby shedding light on the enigmas of withdrawal and relapse at the molecular level (see Chapter 3 ). Epidemiologists have designed and implemented epidemiological surveillance systems that enable policymakers to monitor patterns of drug use in the population ( Chapter 4 ) and that enable researchers to investigate the causes and consequences of drug use and abuse (Chapters 5 and 7 , respectively). Paralleling broader trends in health promotion and disease prevention in the past 20 years, the field of drug abuse prevention has made significant progress in evaluating the effectiveness of interventions implemented in a range of settings including communities, schools, and families (see Chapter 6 ).
Marked gains have also been made in treatment research, including improvements in diagnostic criteria; development of a wide range of treatment interventions and sophisticated methods to assess treatment outcome; and development and approval of Leo-alpha-acetylmethadol (LAAM), a medication for the treatment of opioid dependence. Pharmacological and psychosocial treatments, alone or in combination, have been shown to be effective for drug dependencies, and treatment has been shown to reduce drug use, HIV (human immunodeficiency virus) infection rates, health care costs, and criminal activity (see Chapter 8 ).
Drug abuse researchers have also made major contributions to knowledge in adjacent fields of scientific inquiry. For example, NIDA-sponsored research was the driving force in the identification of morphine-like substances that serve as neurotransmitters in specific neurons located throughout the central and peripheral nervous systems (Orson et al., 1994). Identification of these substances represents a dramatic breakthrough in understanding the mechanisms of pain, reinforcement, and stress. Additionally, the discovery of opioid peptides as neurotransmitters played a key role in the identification of numerous other peptide neurotransmitters (Cooper et al., 1991; Goldstein, 1994; Hokfelt et al., 1995). These discoveries have broadened the understanding of brain function and now
form the basis of many current strategies in the design of new drug treatments for neuropsychiatric disorders. Additionally, drug abuse research has contributed to the development of brain imaging techniques.
Drug abuse research has also provided a major impetus for neuropharmacological research in psychiatry since the late 1950s, when it was discovered that LSD (lysergic acid diethylamide; a hallucinogen that produces psychotic symptoms) affected the brain's serotonin systems (Cooper et al., 1991). That seminal discovery stimulated decades of research in the neuropharmacological basis of behavior and psychiatric disorders. The impact on antipsychotic research has been dramatic. In addition, stimulants (e.g., cocaine and amphetamine) were found to produce a state of paranoid psychosis, resembling schizophrenia, in some people. The actions of stimulants on the brain's dopamine pathways continue to inform researchers of the potential role of those pathways in the treatment, and perhaps the pathophysiology, of schizophrenia (Kahn and Davis, 1995). Drug abuse research also has had an impact on antidepressant research (e.g., the actions of drugs of abuse on the brain's serotonin systems have provided useful models with which to investigate the role of those systems in depression and mania). Depression is a risk factor for treatment failure in smoking cessation (Glassman et al., 1993) and depression-like symptoms are dominant during cocaine withdrawal (DiGregorio, 1990). Consequently, treatment of depression in nicotine and cocaine-dependent individuals has been an area of interest for drug abuse research.
Some drugs that are abused, most notably the opioid analgesics, have essential medical uses. Since its founding, NIDA has been the major supporter of research into brain mechanisms of pain and analgesia, analgesic tolerance, and analgesic pharmacology. The resulting discoveries have led to an understanding of which brain circuits are required to generate pain and pain relief (Wall and Melzack, 1994), have revolutionized the treatment of postoperative and cancer pain (Folly and Interesse, 1986; Car et al., 1992; Jacob et al., 1994), and have led to improved treatments for many other conditions that result in chronic pain (see Chapter 3 ).
VOCABULARY OF DRUG ABUSE
Ordinarily, scientific vocabulary evolves toward greater clarity and precision in response to new empirical discoveries and reconceptualizations. That creative process is evident within each of the disciplines of drug abuse research covered in various chapters of this report. Interestingly, however, the words describing the field as a whole, and connecting each chapter to the next, seem to defy the search for clarity and precision. Does "drug" include alcohol and tobacco? What is "abuse"? Are use and
abuse mutually exclusive categories? Are abuse and dependence mutually exclusive categories? Does use of illicit drugs per se amount to abuse? Does abuse include underage use of nicotine? Is addiction synonymous with dependence?
These ambiguities have persisted for decades because the vocabulary of drug abuse is inevitably influenced by peoples' attitudes and values. If the task were solely a scientific one, precise terminology would have emerged long before now. However, because the choice of words in this field always carries a nonscientific message, scientists themselves cannot always agree on a common vocabulary.
Consider the case of nicotine; from a pharmacological standpoint, nicotine is functionally similar to other psychoactive drugs. However, many researchers and policymakers choose to exclude nicotine from the category of drug. The same is true of alcohol; for example, other terms, such as ''chemical dependency" or "substance abuse," are often used as generic terms encompassing the abuse of nicotine and alcohol as well as abuse of illicit drugs. This semantic strategy is chosen to signify the difference in legal status among alcohol, nicotine, and illicit drugs. In recent years, however, a growing number of researchers have adopted a more inclusive use of the term drug. In the case of nicotine, this move tends to reflect a policy judgment that nicotine should be classified as a drug under the federal Food, Drug and Cosmetic Act.
In the committee's view, the term drug should be understood, in its generic sense, to encompass alcohol and nicotine as well as illicit drugs. It is very important for the general public to recognize that alcohol and nicotine constitute, by far, the nation's two largest drug problems, whether measured in terms of morbidity, mortality, or social cost. Abuse of and dependence on those drugs have serious individual and societal consequences. Continued separation of alcohol, nicotine, and illicit drugs in everyday speech is an impediment to public education, prevention, and therapeutic progress.
Although the committee uses the term drug, in its generic sense, to encompass alcohol and nicotine, the report focuses, at NIDA's request, on research opportunities relating to illicit drugs; research on alcohol and nicotine is discussed only when the scientific inquiries are intertwined. Because the report sometimes ranges more broadly than illicit drugs, however, the committee has adopted several semantic conventions to promote clarity and avoid redundancy. First, the term drug, unmodified, refers to all psychoactive drugs, including alcohol and nicotine. When reference is intended solely to illicit drugs such as heroin, cocaine, and other drugs regulated by the Controlled Substances Act, the committee says so explicitly. Occasionally, to ensure that the intended meaning is clear, the report refers to "illicit drugs and nicotine" or to "illicit drugs
and alcohol," as the case may be. Additionally, the words opiate and opioid are used interchangeably, although opiates are derivative of morphine and opioids are all compounds with morphine-like properties (they may be synthetic and not resemble morphine chemically).
The report employs the standard three-stage conceptualization of drug-taking behavior that applies to all psychoactive drugs, whether licit or illicit. Each stage—use, abuse, dependence—is marked by higher levels of use and increasingly serious consequences. Thus, when the report refers to the "use" of drugs, the term is usually employed in a narrow sense to distinguish it from intensified patterns of use. Conversely, the term "abuse" is used to refer to any harmful use, irrespective of whether the behavior constitutes a "disorder'' in the DSM-IV diagnostic nomenclature (see Appendix C ). When the intent is to emphasize the clinical categories of abuse and dependence, that is made clear.
The committee also draws a clear distinction between patterns of drug-taking behavior, however described, and the harmful consequences of that behavior for the individual and for society. These consequences include the direct, acute effects of drug taking such as a drug-induced toxic psychosis or impaired driving, the effects of repeated drug taking on the user's health and social functioning, and the effects of drug-seeking behavior on the individual and society. It bears emphasizing that adverse consequences can be associated with patterns of drug use that do not amount to abuse or dependence in a clinical sense, although the focus of this report and the committee's recommendations is on the more intensified patterns of use (i.e., abuse and dependence) since they cause the majority of the serious consequences.
DEFINITIONS AND BASIC CONCEPTS
Drug use may be defined as occasional use strongly influenced by environmental factors. Drug use is not a medical disorder and is not listed as such in either of the two most important diagnostic manuals—the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSMIV; APA, 1994); or the International Classification of Diseases (ICD-10; WHO, 1992). (See Appendix C for DSM-IV and ICD-10 diagnostic criteria.) Drug use implies intake for nonmedical purposes; it may or may not be accompanied by clinically significant impairment or distress on a given occasion.
Drug abuse is characterized in DSM-IV as including regular, sporadic, or intensive use of higher doses of drugs leading to social, legal, or interpersonal problems. Like DSM-IV, ICD-10 identifies a nondependent but problematic syndrome of drug use but calls it "harmful use" instead
of abuse. This syndrome is defined by ICD-10 as use resulting in actual physical or psychological harm.
Drug dependence (or addiction) is characterized in both DSM-IV and ICD-10 as drug-seeking behavior involving compulsive use of high doses of one or more drugs, either licit or illicit, for no clear medical indication, resulting in substantial impairment of health and social functioning. Dependence is usually accompanied by tolerance and withdrawal 2 and (like abuse) is generally associated with a wide range of social, legal, psychiatric, and medical problems. Unlike patients with chronic pain or persistent anxiety, who take medication over long periods of time to obtain relief from a specific medical or psychiatric disorder (often with resulting tolerance and withdrawal), persons with dependence seek out the drug and take it compulsively for nonmedical effects.
Tolerance occurs when certain medications are taken repeatedly. With opiates for example, it can be detected after only a few days of use for medical purposes such as the treatment of pain. If the patient suddenly stops taking the drug, a withdrawal syndrome may ensue. Physicians often confuse this phenomenon, referred to as physical dependence, with true addiction. That can lead to withholding adequate medication for the treatment of pain because of the very small risk that addiction with drug-seeking behavior may occur.
As a consequence of its compulsive nature involving the loss of control over drug use, dependence (or addiction) is typically a chronically relapsing disorder (IOM, 1990, 1995; Meter, 1996; O'Brien and McLennan, 1996; McLennan et al., in press). Although individuals with drug dependence can often complete detoxification and achieve temporary abstinence, they find it very difficult to sustain that condition and avoid relapse over time. Most persons who achieve sustained remission do so only after a number of cycles of detoxification and relapse (Dally and Marital, 1992). Relapse is caused by a constellation of biological, family, social, psychological, and treatment factors and is demonstrated by the fact that at least half of former cigarette smokers quit three or more times before they successfully achieve stable remission from nicotine addiction (Schilling, 1992). Similarly, within one year of treatment, relapse occurs in 30-50 percent of those treated for drug dependence, although the level
|
| Tolerance refers to the situation in which repeated administration of a drug at the same dose elicits a diminishing effect or involves the need for an increasing dose to produce the same effect. Withdrawal syndrome is characterized by physical or motivational disturbances when the drug is withdrawn. It is important to emphasize that the phenomena of tolerance, dependence, and withdrawal are not associated uniquely with drugs of abuse, since many medications used clinically that are not addicting (e.g., clonidine, propranolol, tricyclic antidepressants) can produce these types of effects. |
of drug use may not be as high as before treatment (Daley and Marlatt, 1992; McLellan et al., in press). Unlike those who use (or even abuse) drugs, individuals with addiction have a substantially diminished ability to control drug consumption, a factor that contributes to their tendency to relapse.
Another terminological issue arises in relation to the terms addiction and dependence. For some scientists, the proper terms for compulsive drug seeking is addiction, rather than dependence. In their view, addiction more clearly signifies the essential behavioral differences between compulsive use of drugs for their nonmedical effects and the syndrome of "physical dependence" that can develop in connection with repeated medical use. In response, many scientists argue that dependence has been defined in both ICD-10 and DSM-IV to encompass the behavioral features of the disorder and has become the generally accepted term in the diagnostic nomenclature. Moreover, some scientists object to the term addiction on the grounds that it is associated with stigmatizing social images and that a less pejorative term would help to promote public understanding of the medical nature of the condition. The committee has not attempted to resolve this controversy. For purposes of this report, the terms addiction and dependence are used interchangeably.
An inherent aspect of drug addiction is the propensity to relapse. Relapse should not be viewed as treatment failure; addiction itself should be considered a brain disease similar to other chronic and relapsing conditions such as hypertension, diabetes, and asthma (IOM, 1995; O'Brien and McLellan, 1996). In the latter, significant improvement is considered successful treatment even though complete remission or cure is not achieved. In the area of drug abuse, however, many individuals (both lay and professional) expect treatment programs to perform like vaccine programs, where one episode of treatment offers lifetime immunity. Not surprisingly, because of that expectation, people are inevitably disappointed in the relatively high relapse rates associated with most treatments. If, however, addiction is understood as a chronically relapsing brain disease, then—for any one treatment episode—evidence of treatment efficacy would include reduced consumption, longer abstention periods, reduced psychiatric symptoms, improved health, continued employment, and improved family relations. Most of those results are demonstrated regularly in treatment outcome studies.
The idea that drug addiction is a chronic relapsing condition, requiring long-term attention, has been resisted in the United States and in some other countries (Brewley, 1995). Many lay people view drug addiction as a character defect requiring punishment or incarceration. Proponents of the medical model, however, point to the fact that addiction is a distinct morbid process that has characteristics and identifiable signs and
symptoms that affect organ systems (Miller, 1991; Meter, 1996). Characterization of addiction as a brain disease is bolstered by evidence of genetic vulnerability to addiction, physical correlates of its clinical course, physiological changes as a result of repeated drug use, and fundamental changes in brain chemistry as evidenced by brain imaging (Volkow et al., 1993). This is not to say that behavioral, social, and environmental factors are immaterial—they all play a role in onset and outcome, just as they do in heart disease, kidney disease, tuberculosis, or other infectious diseases. Thus, the contemporary understanding of disease fully incorporates the voluntary behavioral elements that lead many people to be skeptical about the applicability of the medical model to drug addiction. In any case, the committee embraces the disease concept, not because it is indisputable but because this paradigm facilitates scientific investigation in many important areas of knowledge, without inhibiting or distorting scientific inquiry in other parts of the field.
IMPORTANCE OF DRUG ABUSE RESEARCH
The widespread prevalence of illicit drug use in the United States is well documented in surveys of households, students, and prison and jail inmates ( Chapter 4 ). Based on the National Household Survey on Drug Abuse (NHSDA), an annual survey presently sponsored by SAMHSA, it was estimated that in 1994, 12.6 million people had used illicit drugs (primarily marijuana) in the past month (SAMHSA, 1995). That figure represents 6 percent of the population 12 years of age or older. 3 The number of heavy drug users, using drugs at least once a week, is difficult to determine. It has been estimated that in 1993 there were 2.1 million heavy cocaine users and 444,000-600,000 heavy heroin users (Rhodes et al., 1995). This population represents a significant burden to society, not only in terms of federal expenditures but also in terms of costs related to the multiple consequences of drug abuse (see Chapter 7 ).
The ultimate aim of the nation's investment in drug abuse research is to enable society to take effective measures to prevent drug use, abuse, and dependence, and thereby reduce its adverse individual and social consequences and associated costs. The adverse consequences of drug abuse are numerous and profound and affect the individual's physical health and psychological and social functioning. Consequences of drug abuse include increased rates of HIV infection and tuberculosis (TB); education and vocational impairment; developmental harms to children of
|
| It is important to note that the total number of users results from the rates of use in different age groups in the population and from the demographic structure of the population. The actual number of users may increase while the rates of use are declining. |
drug-using parents associated with fetal exposure or maltreatment and neglect; and increased violence (see Chapter 7 ). It now appears that injection drug use is the leading risk factor for new HIV infection in the United States (Holmberg, 1996). Most (80 percent) HIV-infected heterosexual men and women who do not use injection drugs have been infected through sexual contact with HIV-infected injection drug users (IUDs). Thus, it is not surprising that the geographic distribution of heterosexual AIDS cases has been essentially the same as the distribution of male injection drug users' AIDS cases (Holmberg, 1996) Further, the IUDs-associated HIV epidemic in men is reflected in the heterosexual epidemic in women, which is reflected in HIV infection in children (CDC, 1995). Nearly all children who acquire HIV infection do so prenatal (see Chapter 7 ).
The extent of the impact of drug use and abuse on society is evidenced by its enormous economic burden. In 1990, illicit drug abuse is estimated to have cost the United States more than $66 billion. When the cost of illicit drug use and abuse is tallied with that of alcohol and nicotine ( Table 1.1 ), the collective cost of drug use and abuse exceeds the estimated annual $117 billion cost of heart disease and the estimated annual $104 billion cost of cancer (AHA, 1992; ACS, 1993; D. Rice, University of California at San Francisco, personal communication, 1995).
As noted above, the federal government accounts for a large segment of the societal expenditure on illicit drug abuse control—spending more than $13.3 billion in FY 1995 (ONDCP, 1996). About two-thirds was devoted to interdiction, intelligence, incarceration, and other law enforcement activities. Research, however, accounts for only 4 percent of federal outlays, a percentage that has remained virtually unchanged since 1981 (ONDCP, 1996) ( Figure 1.1 ). Given the social costs of illicit drug abuse and the enormity of the federal investment in prevention and control, research into the causes, consequences, treatment, and prevention of drug abuse should have a higher priority. Enhanced support for drug abuse research would be a socially sound investment, because scientific research can be expected to generate new and improved treatments, as well as prevention and control strategies that can help reduce the enormous social burden associated with drug abuse.
THE CONTEXT OF DRUG ABUSE RESEARCH
In the chapters that follow, the committee identifies research initiatives that seem most promising and most likely to lead to successful efforts to reduce drug abuse and its associated social costs. Although the yield from these initiatives will depend largely on the creativity and skill of scientists, the many contextual factors that will also have a major bear-
TABLE 1.1 Estimated Economic Costs (million dollars) of Drug Abuse, 1990
|
| Illicit Drugs | Alcohol | Nicotine |
| Total | $66,873 | $98,623 | $91,269 |
| Core Costs | 14,602 | 80,763 | 91,269 |
| Direct | 3,197 | 10,512 | 39,130 |
| Mental health/specialty organizations | 867 | 3,469 | — |
| Short-stay hospitals | 1,889 | 4,589 | 21,072 |
| Office-based physicians | 88 | 240 | 12,251 |
| Other professional services | 32 | 329 | — |
| Prescription drugs | — | — | 1,469 |
| Nursing homes | — | 1,095 | 3,858 |
| Home health services | — | — | 480 |
| Support costs | 321 | 790 | — |
| Indirect | 11,405 | 70,251 | 52,139 |
| Morbidity | 7,997 | 36,627 | 6,603 |
| Mortality | 3,408 | 33,624 | 45,536 |
| Other Related Costs | 45,989 | 15,771 | — |
| Direct | 18,043 | 10,436 | — |
| Crime | 18,035 | 5,807 | — |
| Motor vehicle crashes | — | 3,876 | — |
| Fire destruction | — | 633 | — |
| Social welfare administration | 8 | 120 | — |
| Indirect | 27,946 | 5,335 | — |
| Victims of crime | 1,042 | 576 | — |
| Incarceration | 7,813 | 4,75 | — |
| Crime careers | 19,091 | — | — |
| AIDS | 6,282 | — | — |
| Fetal Alcohol Syndrome |
| 2,089 | — |
| NOTE: 1990 costs for illicit drugs and alcohol abuse are based on socioeconomic indexes applied to 1985 estimates (Rice et al., 1990; cigarette direct smoking costs are deflated from 1993 direct cost estimates (MMWR, 1994); cigarette indirect costs are from Rice et al., 1992. Amounts spent for other professional services are included in office-based physicians' costs. Value of goods and services lost by individuals unable to perform their usual activities because of drug abuse or unable to perform them at a level of full effectiveness (Rice et al., 1990). Present value of future earnings lost, illicit drugs and alcohol discounted at 6 percent, nicotine discounted at 4 percent. SOURCE: D. Rice, University of California at San Francisco, personal communication (1995). | |||
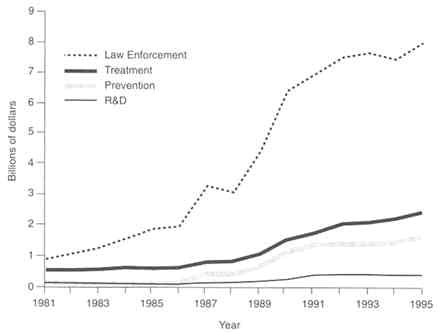
FIGURE 1.1 Federal drug control budget trends (1981-1995). NOTE: Figures are in current dollars. SOURCE: ONDCP (1996).
ing on the payoff from scientific inquiry cannot be ignored. The committee has identified six major factors that, if successfully addressed, could optimize the gains made in each area of drug abuse research: stable funding; use of a comprehensive public health framework; wider acceptance of a medical model of drug dependence; better translation of research findings into practice; raising the status of drug abuse research; and facilitating interdisciplinary research.
Stable Funding
A stable level of funding in any area of biomedical research is needed to sustain and build on research accomplishments, to retain a cadre of experts in a field, and to attract young investigators. Drug abuse research, in comparison with many other research venues, has not enjoyed consistent federal support (IOM, 1990, 1995; see also Appendix B ). The field has suffered from difficulties in recruiting and retaining young researchers and clinicians and in maintaining a stable research infrastructure (IOM, 1995). Society's capacity to contain and manage drug abuse
depends upon a stable, long-term investment in research. The vicissitudes in federal research funding often reflect changing currents in public opinion toward drugs and drug users ( Appendix B ). However, drug abuse will not disappear; it is an endemic social and public health problem. The nation must commit itself to a sustained effort. The social investment in research is an investment in "human capital" that must be sustained over the long term in order to reap the expected gains. An investment in this field is squandered if researchers who have been recruited and trained in drug abuse research are drawn to other fields because of uncertainty about the stability of future funding.
Adoption of a Comprehensive Public Health Framework
The social impact of drug abuse research can be enhanced significantly by conceptualizing goals and priorities within a comprehensive public health framework (Goldstein, 1994). All too often, public discourse about drug abuse is characterized by such unnecessary and fruitless disputes as whether drug abuse should be viewed as a social and moral problem or a health problem, whether the drug problem can best be solved by law enforcement or by medicine, whether priority should be placed on reducing supply or reducing demand, and so on. The truth is that these dichotomies oversimplify a brain disease impacted by a complex set of behaviors and a diverse array of potentially useful social responses. Forced choices of this nature also tend to inhibit or foreclose potentially useful research strategies. Confusion about social goals can lead to confusion about research priorities and can obscure the links between investigations viewing the subject through different lenses.
Some issues tend to recur. A prominent dispute centers on whether preventing drug use is important in itself or whether society should be more concerned with abuse or with the harmful consequences of use. The answer, of course, is that such a forced choice obscures, rather than clarifies, the issues. From a public health standpoint, drug use is a risk factor; the significance of use (whether of alcohol, nicotine, or illicit drugs) lies in the risk of harm associated with it (e.g., fires from smoking, impaired driving from alcohol or illicit drugs, or developmental setbacks) and in the risk that use will intensify, escalating to abuse or dependence. Those risks vary widely in relation to drug, user characteristics, social context, etc. Attention to the consequences of use and to the risk of escalation helps to set priorities (for research and policy) and provides a framework for assessing the impact of different interventions.
From a public policy standpoint, arguments about goals and priorities are fraught with controversy. From the standpoint of research strategy, however, the key lies in asking the right questions (e.g., What influ-
ences the pathways from use, to abuse, to dependence? What are the effects of needle exchange programs on illicit drug use and on HIV disease?) and in generating the knowledge required to facilitate informed policy debate. The main virtues of a comprehensive public health approach are that it helps to disentangle scientific questions from policy questions and that it encompasses all of the pertinent empirical questions, including the causes and consequences of use, abuse, and dependence, as well as the efficacy and cost of all types of interventions. In sum, the social payoff from drug abuse research can be enhanced substantially by integrating diverse strands of inquiry within a public health framework.
Acceptance of a Medical Model of Drug Dependence
Drug dependence is a chronic, relapsing brain disease that, like other diseases, can be evaluated and treated with the standard tools of medicine, including efforts in prevention, diagnosis, and treatment with medications and behavioral or psychosocial therapies. Unfortunately, the medical model of dependence is not universally accepted by health professionals and others in the treatment community; it is widely rejected within the law enforcement community and often by the public at large, which tends to view the complex and varied patterns of use, abuse, and dependence as an undifferentiated behavior rather than a medical problem.
Resistance to the medical model takes many forms. One is resistance to pharmacotherapies, such as methadone, that are seen as substituting licit drugs for illicit drugs without changing drug-taking behavior. Conversely, treatment approaches that adopt a rigid drug-free strategy preclude the use of medications for patients with other psychiatric disorders that are easily treated by pharmacotherapeutic approaches. On a subtler level, resistance to the use of pharmacotherapies is evidenced by the routine use of inadequate doses of methadone (D'Aunno and Vaughn, 1992). Finally, for others, all forms of drug abuse signify a failure of willpower or a moral weakness requiring punishment, incarceration, or moral education rather than treatment (Anglin and Hser, 1992).
Resistance to the medical model of drug dependence presents numerous barriers to research. Clinical researchers experience difficulty in soliciting participation by both treatment program administrators and patients, who are sometimes mistrustful of researchers' motives. If research involves a medication that is itself prone to abuse, there are additional regulatory requirements for drug scheduling, storage, and record keeping that act to discourage investigation (see Chapter 10 ; IOM, 1995). The ever-present threat of inappropriate intrusion by law enforcement agents has a chilling effect on treatment research (McDuff et al., 1993). All barri-
ers to inquiry, irrespective of whether they are legal or social in origin, raise the cost of research and discourage researchers from entering the field. Additionally, those barriers diminish the likelihood that a pharmaceutical company will invest in the development of antiaddiction medications (IOM, 1995). 4 Broader acceptance of the medical model of drug dependence would provide an incentive for researchers and clinicians to enter this field of research. Over time, a developing consensus in support of the medical model could facilitate common discourse, help to shape a shared research agenda within a public health framework, and diminish tensions between the research and treatment communities and the criminal justice system.
Better Translation of Research Findings into Practice and Policy
To benefit society, new research findings must be disseminated adequately to treatment providers, educators, law enforcement officials, and community leaders. In the case of prevention practices, it is often difficult for communities to change entrenched policies, particularly when combined with political imperatives for action to counteract drug abuse. In the case of treatment, technology transfer is impeded by the heterogeneity of providers and their marginalization at the outskirts of the medical community (see IOM, 1990, 1995; see also Chapter 8 ). Physicians and psychiatrists are seldom employed by specialized drug treatment facilities (approximately one-quarter employ medical doctors), and treatment is delivered by counselors whose training and supervision vary greatly and who have little access to and understanding of research results (Ball and Ross, 1991; Batten et al., 1993). These factors not only impede the transfer of research findings to the field but also impede communication from the field to the laboratory so that research designs can be modified in response to clinical realities (Pentz, 1994). Thus, there is a real need for bidirectional communication, from bench to bedside and back to the basic scientist (IOM, 1994).
The committee is aware, however, of recent technology transfer efforts in the field such as the Treatment Improvement Protocol Series, an initiative to establish guidelines for drug abuse treatment with an emphasis on incorporating research findings (SAMHSA, 1993), and the Prevention Enhancement Protocol System, a process implemented by the Center
|
| In recognition of the barriers to pharmaceutical company investment in this area of drug development, Congress in 1990 created NIDA's Medications Development Division (IOM, 1990) to stimulate the discovery and development of new medications for the treatment of drug abuse. |
for Substance Abuse Prevention in which scientists and practitioners develop protocols to identify and evaluate the strength of evidence on topics related to prevention interventions. Similar efforts will be invaluable for communicating and integrating research results to the treatment community.
Research frequently results in product development leading to changes in operations and an overall enhancement of the value of the enterprise. For example, in the pharmaceutical industry research often leads to the development of new medications or devices. In the public sector, however, research is often divorced from the implementation of findings and development. Research is often more basic than applied, and the fruits of research are not realized by the government, but by the private sector. Although that approach may be appropriate, it is unfortunately not always the most productive strategy for advancing research, knowledge, and product development. That is particularly true in the development of medications for opiate and cocaine addictions, where there is a great need for commitment from the private sector. However, many obstacles prevent active involvement of the pharmaceutical industry in this area of research and development (IOM, 1995).
A similar problem arises in relation to policymaking. Because debates about drug policy tend to be so highly polarized and politicized, research findings are often distorted, or selectively deployed, for rhetorical purposes. Researchers cannot prevent this practice, which is a common feature of political debate in a democratic society. However, researchers and their sponsors should not be indifferent to the disconnect between policy discourse and science. Researchers should establish and support institutional mechanisms for communicating an important message to policymakers and to the general public. Scientific research has produced a solid, and growing, body of knowledge about drug abuse and about the efficacy of various interventions that aim to prevent and control it. As long as drug abuse remains a poorly understood social problem, policy will be based mainly on wish and supposition; steps should be taken to educate policymakers about the scientific and technological advances in addiction research. Only then will it be possible for policymaking to support legislation that adequately funds new research and applies research findings. To some extent, persisting failure to reap the fruits of drug abuse research is attributable to the low visibility of the field—a problem to which the discussion now turns.
Raising the Status of Drug Abuse Research
Drug abuse research is often an undervalued area of inquiry, and most scientists and clinicians choose other disciplines in which to develop
their careers. Compared with other fields of research, investigators in drug abuse are often paid less, have less prestige among their peers, and must contend with the unique complexities of performing research in this area (e.g., regulations on controlled substances) (see IOM, 1995). The overall result is an insufficient number of basic and clinical researchers. IOM has recently begun a study, funded by the W. M. Keck Foundation of Los Angeles, to develop strategies to raise the status of drug abuse research. 5
Weak public support for this field of study is evident in unstable federal funding (see above), a lack of pharmaceutical industry investment in the development of antiaddiction medications (IOM, 1995), and inadequate funding for research training (IOM, 1995). NIDA's FY 1994 training budget, which is crucial to the flow of young researchers into the field, was about 2 percent of its extramural research budget, a percentage substantially lower than the overall National Institutes of Health (NIH) training budget, which averages 4.8 percent of its extramural research budget.
Beyond funding problems, investigators face a host of barriers to research: research subjects may pose health risks (e.g., TB, HIV/AIDS, and other infectious diseases), may be noncompliant, may deny their drug abuse problems, and may be involved in the criminal justice system. Even when research is successful and points to improvements in service delivery, the positive outcome may not be translated into practice or policy. For example, more than a year after the Food and Drug Administration's (FDA's) approval of levo-alpha-acetylmethadol (LAAM) as the first new medication for the treatment of opiate dependence in over 20 years, fewer than 1,000 patients nationwide actually had received the medication (IOM, 1995). More recently, scientific evidence regarding the beneficial effects of needle exchange programs (NRC, 1995) has received inadequate attention. Continuing indifference to scientific progress in drug abuse research inevitably depresses the status of the field, leading in turn to difficulties in recruiting new investigators.
Increasing Interdisciplinary Research
The breadth of expertise needed in drug abuse research spans many disciplines, including the behavioral sciences, pharmacology, medicine, and the neurosciences, and many fields of inquiry, including etiology, epidemiology, prevention, treatment, and health services research. Aspects of research relating to drug use tend to draw on developmental perspectives and to focus on general population samples in community settings, especially schools. Aspects of research relating to abuse and de-
|
| The report on raising the profile of drug abuse will be published in the Fall of 1996. |
pendence tend to be more clinical in nature, drawing on psychopathological perspectives. Additionally, a full account of any aspect of drug-taking behavior must also reflect an understanding of social context. The rich interplay between neuroscience and behavioral research and between basic and clinical research poses distinct challenges and opportunities.
Unfortunately, research tends to be fragmented within disciplinary boundaries. The difficulties in conducting successful interdisciplinary research are well known. Funds for research come from many separate agencies, such as the NIDA, NIMH, and SAMHSA. These agencies all have different programmatic emphases as they attempt to shape the direction of research in their respective fields. In times of funding constraints, agencies may be less inclined to fund projects at the periphery of their interests.
Additionally, NIH study sections, which rank grant proposals, are discipline specific, making it difficult for interdisciplinary proposals to ''qualify" (i.e., receive a high rank) for funding. Another problem is that the most advanced scientific literature tends to be compartmentalized within discipline or subject matter categories, making it difficult for scientists to see the whole field. The problem is exacerbated by what Tonry (1990) has called "fugitive literatures," studies carried out by private sector research firms or independent research agencies and available only in reports submitted to the sponsoring agency.
In light of lost opportunities for collaboration and interdisciplinary research, IOM (1995) previously recommended the creation and expansion of comprehensive drug abuse centers to coordinate all aspects of drug abuse research, training, and treatment. The field of drug abuse research presents a real opportunity to bridge the intellectual divide between the behavioral and neuroscience communities and to overcome the logistical impediments to interdisciplinary research.
INVESTING WISELY IN DRUG ABUSE RESEARCH
This report sets forth drug abuse research initiatives for the next decade based on a thorough assessment of what is now known and a calculated judgment about what initiatives are most likely to advance our knowledge in useful ways. This report is not meant to be a road map or tactical battle plan, but is best regarded as a strategic outline. Within each discipline of drug abuse research, the committee has highlighted priorities for future research. However, the committee did not make any attempt to prioritize recommendations across varied disciplines and fields of research. Prudent research planning must respond to newly emerging opportunities and needs while maintaining a steady commitment to the
achievement of long-term objectives. The ability to respond to new goals and needs may be the real challenge for the field of drug abuse research.
Drug abuse research is an important public investment. The ultimate aim of that investment is to reduce the enormous social costs attributable to drug abuse and dependence. Of course, drug abuse research must also compete for funding with research in other fields of public health, research in other scientific domains, and other pressing public needs. Recognizing the scarcity of resources, the committee has also considered ways in which the research effort can be harnessed most effectively to increase the yield per dollar invested. These include stable funding, use of a comprehensive public health framework, wider acceptance of a medical model of drug dependence, better translation of research findings into practice and policy, raising the status of drug abuse research, and facilitating interdisciplinary research.
The committee notes that there have been major accomplishments in drug abuse research over the past 25 years and commends NIDA for leading that effort. The committee is convinced that the field is on the threshold of significant advances, and that a sustained research effort will strengthen society's capacity to reduce drug abuse and to ameliorate its adverse consequences.
ORGANIZATION OF THE REPORT
This report sets forth a series of initiatives in drug abuse research. 6 Each chapter of the report covers a segment of the field, describes selected accomplishments, and highlights areas that seem ripe for future research. As noted, the committee has not prioritized areas for future research but, instead, has identified those areas that most warrant further exploration.
Chapter 2 describes behavioral models of drug abuse and demonstrates how the use of behavioral procedures has given researchers the ability to measure drug-taking objectively and to study the development, maintenance, and consequences of that behavior. Chapter 3 discusses drug abuse within the context of neurotransmission; it describes neurobiological advances in drug abuse research and provides the foundation for the current understanding of addiction as a brain disease. The epidemiological information systems designed to gather information on drug use in the United States are identified in Chapter 4 . The data collected from the systems provide an essential foundation for systematic study of
|
| As noted earlier, the primary focus of the report is research on illicit drugs, such as heroin and cocaine. Research on alcohol and nicotine is cited in the text where it has illuminated our knowledge of illicit drug abuse. |
the etiology and consequences of drug abuse, which are addressed, respectively, in Chapters 5 and 7 . Chapter 6 addresses the efficacy of interventions designed to prevent drug abuse. The effectiveness of drug abuse treatment and the difficulties in treating special populations of drug users are discussed in Chapter 8 , while the impact of managed care on access, costs, utilization, and outcomes of treatment is addressed in Chapter 9 . Finally, Chapter 10 discusses the effects of drug control on public health and identifies areas for policy-relevant research.
Specific recommendations appear in each chapter. Although these recommendations reflect the committee's best judgment regarding priorities within the specific domains of research, the committee did not identify priorities or rank recommendations for the entire field of drug abuse research. Opportunities for advancing knowledge exist in all domains. It would be a mistake to invest too narrowly in a few fields of inquiry. At the present time, soundly conceived research should be pursued in all domains along the lines outlined in this report.
ACS (American Cancer Society). 1993. Cancer Facts and Figures, 1993 . Washington, DC: ACS.
AHA (American Heart Association). 1992. 1993 Heart and Stroke Fact Statistics . Dallas, TX: AHA.
Anglin MD, Hser Y. 1992. Treatment of drug abuse. In: Watson RR, ed. Drug Abuse Treatment. Vol. 3, Drug and Alcohol Abuse Reviews . New York: Humana Press.
APA (American Psychiatric Association). 1994. Diagnostic and Statistical Manual of Mental Disorders . 4th ed. Washington, DC: APA.
Ball JC, Ross A. 1991. The Effectiveness of Methadone Maintenance Treatment . New York: Springer-Verlag.
Batten H, Horgan CM, Prottas J, Simon LJ, Larson MJ, Elliott EA, Bowden ML, Lee M. 1993. Drug Services Research Survey Final Report: Phase I . Contract number 271-90-8319/1. Submitted to the National Institute of Drug Abuse. Waltham, MA: Bigel Institute for Health Policy, Brandeis University.
Brewley T. 1995. Conversation with Thomas Brewley. Addiction 90:883-892.
Carr DB, Jacox AK, Chapman CR, et al. 1992. Acute Pain Management: Operative or Medical Procedures and Trauma. Clinical Practice Guidelines . AHCPR Publication No. 92-0032. Rockville, MD: U.S. Public Health Service, Agency for Health Care Policy and Research.
CDC (Centers for Disease Control and Prevention). 1995. HIV/AIDS Surveillance Report 7(2).
Cooper JR, Bloom FE, Roth RH. 1991. The Biochemical Basis of Neuropharmacology . 6th ed. New York: Oxford University Press.
Daley DC, Marlatt GA. 1992. Relapse prevention: Cognitive and behavioral interventions. In: Lowinson JH, Ruiz P, Millman RB, Langrod JG, eds. Substance Abuse: A Comprehensive Textbook . Baltimore: Williams and Wilkins.
D'Aunno T, Vaughn TE. 1992. Variation in methadone treatment practices. Journal of the American Medical Association 267:253-258.
DiGregorio GJ. 1990. Cocaine update: Abuse and therapy. American Family Physician 41(1):247-250.
Foley KM, Inturrisi CE, eds. 1986. Opioid Analgesics in the Management of Clinical Pain. Advances in Pain Research and Therapy. Vol. 8. New York: Raven Press.
GAO (General Accounting Office). 1992. Drug Abuse Research: Federal Funding and Future Needs . GAO/PEMD-92-5. Washington, DC: GAO.
Glassman AH, Covey LS, Dalack GW, Stetner F, Rivelli SK, Fleiss J, Cooper TB. 1993. Smoking cessation, clonidine, and vulnerability to nicotine among dependent smokers. Clinical Pharmacology and Therapeutics 54(6):670-679.
Goldstein A. 1994. Addiction: From Biology to Drug Policy . New York: W.H. Freeman.
Hokfelt TGM, Castel MN, Morino P, Zhang X, Dagerlind A. 1995. General overview of neuropeptides. In: Bloom FE, Kupfer DJ, eds. Psychopharmacology: Fourth Generation of Progress . New York: Raven Press. Pp. 483-492.
Holmberg SD. 1996 . The estimated prevalence and incidence of HIV in 96 large U.S. metropolitan areas . American Journal of Public Health 86(5):642-654.
IOM (Institute of Medicine). 1990. Treating Drug Problems . Washington, DC: National Academy Press.
IOM (Institute of Medicine). 1994. AIDS and Behavior: An Integrated Approach . Washington, DC: National Academy Press.
IOM (Institute of Medicine). 1995. The Development of Medications for the Treatment of Opiate and Cocaine Addictions. Washington, DC: National Academy Press.
Jacox A, Carr DB, Payne R, et al. 1994. Management of Cancer Pain. Clinical Practice Guideline . AHCPR Publication No. 94-0592. Rockville, MD: U.S. Public Health Service, Agency for Health Care Policy and Research.
Kahn RS, Davis KL. 1995. New developments in dopamine and schizophrenia. In: Bloom FE, Kupfer DJ, eds. Psychopharmacology: Fourth Generation of Progress . New York: Raven Press. Pp. 1193-1204.
McDuff DR, Schwartz RP, Tommasello A, Tiegel S, Donovan T, Johnson JL. 1993. Outpatient benzodiazepine detoxification procedure for methadone patients. Journal of Substance Abuse Treatment 10:297-302.
McLellan AT, Metzger DS, Alterman Al, Woody GE, Durell J, O'Brien CP. In press. Is addiction treatment "worth it"? Public health expectations, policy-based comparisons. Milbank Quarterly .
Meyer R. 1996. The disease called addiction: Emerging evidence in a 200-year debate. Lancet 347:162-166.
Miller NS. 1991. Drug and alcohol addiction as a disease. In: Miller NS, ed. Comprehensive Handbook of Drug and Alcohol Addiction . New York: Marcel Dekker.
MMWR (Morbidity and Mortality Weekly Report). 1994. Medical care expenditures attributable to cigarette smoking, United States, 1993. Morbidity and Mortality Weekly Report 43(26):469-472.
NRC (National Research Council). 1995. Preventing HIV Transmission: The Role of Sterile Needles and Bleach . Washington, DC: National Academy Press.
O'Brien CP, McLellan AT. 1996. Myths about the treatment of addiction. Lancet 347:237-240.
Olson GA, Olson RD, Kastin AJ. 1994. Endogenous opiates, 1993. Peptides 15:1513-1556.
ONDCP (Office of National Drug Control Policy). 1996. National Drug Control Strategy . Washington, DC: ONDCP.
Pentz M. 1994. Directions for future research in drug abuse prevention. Preventive Medicine 23:646-652.
Rhodes W, Scheiman P, Pittayathikhun T, Collins L, Tsarfaty V. 1995. What America's Users Spend on Illegal Drugs, 1988-1993 . Prepared for the Office of National Drug Control Policy, Washington, DC.
Rice DP, Kelman S, Miller LS, Dunmeyer S. 1990. The Economic Costs of Alcohol and Drug Abuse and Mental Illness: 1985 . DHHS Publication No. (ADM) 90-1694. San Francisco: University of California, Institute for Health and Aging.
Rice DP, Max W, Novotny T, Shultz J, Hodgson T. 1992. The Cost of Smoking Revisited: Preliminary Estimates . Paper presented at the American Public Health Association Annual Meeting, November 23, 1992. Washington, DC.
SAMHSA (Substance Abuse and Mental Health Services Administration). 1993. Improving Treatment for Drug-Exposed Infants: Treatment Improvement Protocol (TIP) Series . Washington, DC: U.S. Department of Health and Human Services.
SAMHSA (Substance Abuse and Mental Health Services Administration). 1995. National Household Survey on Drug Abuse: Population Estimates 1994 . Washington, DC: U.S. Department of Health and Human Services.
Schelling TC. 1992 . Addictive drugs: The cigarette experience. Science 255:431-433.
Tonry M. 1990. Research on drugs and crime. In: Morris N, Tonry M, eds. Drugs and Crime . Vol. 13 . Chicago: University of Chicago Press.
Volkow ND, Fowler JS, Wang G-J, Hitzemann R, Logan J, Schlyer DJ, Dewey SI, Wolf AD. 1993. Decreased dopamine D2 receptor availability is associated with reduced frontal metabolism in cocaine abusers. Synapse 14:169-177.
Wall PD, Melzack R. 1994. Textbook of Pain . 3rd ed. Edinburg: Churchill-Livingstone.
WHO (World Health Organization). 1992. International Statistical Classification of Diseases and Related Health Problems . Tenth Revision. Geneva: WHO.
Drug abuse persists as one of the most costly and contentious problems on the nation's agenda. Pathways of Addiction meets the need for a clear and thoughtful national research agenda that will yield the greatest benefit from today's limited resources.
The committee makes its recommendations within the public health framework and incorporates diverse fields of inquiry and a range of policy positions. It examines both the demand and supply aspects of drug abuse.
Pathways of Addiction offers a fact-filled, highly readable examination of drug abuse issues in the United States, describing findings and outlining research needs in the areas of behavioral and neurobiological foundations of drug abuse. The book covers the epidemiology and etiology of drug abuse and discusses several of its most troubling health and social consequences, including HIV, violence, and harm to children.
Pathways of Addiction looks at the efficacy of different prevention interventions and the many advances that have been made in treatment research in the past 20 years. The book also examines drug treatment in the criminal justice setting and the effectiveness of drug treatment under managed care.
The committee advocates systematic study of the laws by which the nation attempts to control drug use and identifies the research questions most germane to public policy. Pathways of Addiction provides a strategic outline for wise investment of the nation's research resources in drug abuse. This comprehensive and accessible volume will have widespread relevance—to policymakers, researchers, research administrators, foundation decisionmakers, healthcare professionals, faculty and students, and concerned individuals.
READ FREE ONLINE
Welcome to OpenBook!
You're looking at OpenBook, NAP.edu's online reading room since 1999. Based on feedback from you, our users, we've made some improvements that make it easier than ever to read thousands of publications on our website.
Do you want to take a quick tour of the OpenBook's features?
Show this book's table of contents , where you can jump to any chapter by name.
...or use these buttons to go back to the previous chapter or skip to the next one.
Jump up to the previous page or down to the next one. Also, you can type in a page number and press Enter to go directly to that page in the book.
Switch between the Original Pages , where you can read the report as it appeared in print, and Text Pages for the web version, where you can highlight and search the text.
To search the entire text of this book, type in your search term here and press Enter .
Share a link to this book page on your preferred social network or via email.
View our suggested citation for this chapter.
Ready to take your reading offline? Click here to buy this book in print or download it as a free PDF, if available.
Get Email Updates
Do you enjoy reading reports from the Academies online for free ? Sign up for email notifications and we'll let you know about new publications in your areas of interest when they're released.
Change Password
Your password must have 6 characters or more:.
- a lower case character,
- an upper case character,
- a special character
Password Changed Successfully
Your password has been changed
Create your account
Forget yout password.
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password
Forgot your Username?
Enter your email address below and we will send you your username
If the address matches an existing account you will receive an email with instructions to retrieve your username
- June 01, 2024 | VOL. 181, NO. 6 CURRENT ISSUE pp.461-564
- May 01, 2024 | VOL. 181, NO. 5 pp.347-460
- April 01, 2024 | VOL. 181, NO. 4 pp.255-346
- March 01, 2024 | VOL. 181, NO. 3 pp.171-254
- February 01, 2024 | VOL. 181, NO. 2 pp.83-170
- January 01, 2024 | VOL. 181, NO. 1 pp.1-82
The American Psychiatric Association (APA) has updated its Privacy Policy and Terms of Use , including with new information specifically addressed to individuals in the European Economic Area. As described in the Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences.
Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.
Substance Use Disorders and Addiction: Mechanisms, Trends, and Treatment Implications
- Ned H. Kalin , M.D.
Search for more papers by this author
The numbers for substance use disorders are large, and we need to pay attention to them. Data from the 2018 National Survey on Drug Use and Health ( 1 ) suggest that, over the preceding year, 20.3 million people age 12 or older had substance use disorders, and 14.8 million of these cases were attributed to alcohol. When considering other substances, the report estimated that 4.4 million individuals had a marijuana use disorder and that 2 million people suffered from an opiate use disorder. It is well known that stress is associated with an increase in the use of alcohol and other substances, and this is particularly relevant today in relation to the chronic uncertainty and distress associated with the COVID-19 pandemic along with the traumatic effects of racism and social injustice. In part related to stress, substance use disorders are highly comorbid with other psychiatric illnesses: 9.2 million adults were estimated to have a 1-year prevalence of both a mental illness and at least one substance use disorder. Although they may not necessarily meet criteria for a substance use disorder, it is well known that psychiatric patients have increased usage of alcohol, cigarettes, and other illicit substances. As an example, the survey estimated that over the preceding month, 37.2% of individuals with serious mental illnesses were cigarette smokers, compared with 16.3% of individuals without mental illnesses. Substance use frequently accompanies suicide and suicide attempts, and substance use disorders are associated with a long-term increased risk of suicide.
Addiction is the key process that underlies substance use disorders, and research using animal models and humans has revealed important insights into the neural circuits and molecules that mediate addiction. More specifically, research has shed light onto mechanisms underlying the critical components of addiction and relapse: reinforcement and reward, tolerance, withdrawal, negative affect, craving, and stress sensitization. In addition, clinical research has been instrumental in developing an evidence base for the use of pharmacological agents in the treatment of substance use disorders, which, in combination with psychosocial approaches, can provide effective treatments. However, despite the existence of therapeutic tools, relapse is common, and substance use disorders remain grossly undertreated. For example, whether at an inpatient hospital treatment facility or at a drug or alcohol rehabilitation program, it was estimated that only 11% of individuals needing treatment for substance use received appropriate care in 2018. Additionally, it is worth emphasizing that current practice frequently does not effectively integrate dual diagnosis treatment approaches, which is important because psychiatric and substance use disorders are highly comorbid. The barriers to receiving treatment are numerous and directly interact with existing health care inequities. It is imperative that as a field we overcome the obstacles to treatment, including the lack of resources at the individual level, a dearth of trained providers and appropriate treatment facilities, racial biases, and the marked stigmatization that is focused on individuals with addictions.
This issue of the Journal is focused on understanding factors contributing to substance use disorders and their comorbidity with psychiatric disorders, the effects of prenatal alcohol use on preadolescents, and brain mechanisms that are associated with addiction and relapse. An important theme that emerges from this issue is the necessity for understanding maladaptive substance use and its treatment in relation to health care inequities. This highlights the imperative to focus resources and treatment efforts on underprivileged and marginalized populations. The centerpiece of this issue is an overview on addiction written by Dr. George Koob, the director of the National Institute on Alcohol Abuse and Alcoholism (NIAAA), and coauthors Drs. Patricia Powell (NIAAA deputy director) and Aaron White ( 2 ). This outstanding article will serve as a foundational knowledge base for those interested in understanding the complex factors that mediate drug addiction. Of particular interest to the practice of psychiatry is the emphasis on the negative affect state “hyperkatifeia” as a major driver of addictive behavior and relapse. This places the dysphoria and psychological distress that are associated with prolonged withdrawal at the heart of treatment and underscores the importance of treating not only maladaptive drug-related behaviors but also the prolonged dysphoria and negative affect associated with addiction. It also speaks to why it is crucial to concurrently treat psychiatric comorbidities that commonly accompany substance use disorders.
Insights Into Mechanisms Related to Cocaine Addiction Using a Novel Imaging Method for Dopamine Neurons
Cassidy et al. ( 3 ) introduce a relatively new imaging technique that allows for an estimation of dopamine integrity and function in the substantia nigra, the site of origin of dopamine neurons that project to the striatum. Capitalizing on the high levels of neuromelanin that are found in substantia nigra dopamine neurons and the interaction between neuromelanin and intracellular iron, this MRI technique, termed neuromelanin-sensitive MRI (NM-MRI), shows promise in studying the involvement of substantia nigra dopamine neurons in neurodegenerative diseases and psychiatric illnesses. The authors used this technique to assess dopamine function in active cocaine users with the aim of exploring the hypothesis that cocaine use disorder is associated with blunted presynaptic striatal dopamine function that would be reflected in decreased “integrity” of the substantia nigra dopamine system. Surprisingly, NM-MRI revealed evidence for increased dopamine in the substantia nigra of individuals using cocaine. The authors suggest that this finding, in conjunction with prior work suggesting a blunted dopamine response, points to the possibility that cocaine use is associated with an altered intracellular distribution of dopamine. Specifically, the idea is that dopamine is shifted from being concentrated in releasable, functional vesicles at the synapse to a nonreleasable cytosolic pool. In addition to providing an intriguing alternative hypothesis underlying the cocaine-related alterations observed in substantia nigra dopamine function, this article highlights an innovative imaging method that can be used in further investigations involving the role of substantia nigra dopamine systems in neuropsychiatric disorders. Dr. Charles Bradberry, chief of the Preclinical Pharmacology Section at the National Institute on Drug Abuse, contributes an editorial that further explains the use of NM-MRI and discusses the theoretical implications of these unexpected findings in relation to cocaine use ( 4 ).
Treatment Implications of Understanding Brain Function During Early Abstinence in Patients With Alcohol Use Disorder
Developing a better understanding of the neural processes that are associated with substance use disorders is critical for conceptualizing improved treatment approaches. Blaine et al. ( 5 ) present neuroimaging data collected during early abstinence in patients with alcohol use disorder and link these data to relapses occurring during treatment. Of note, the findings from this study dovetail with the neural circuit schema Koob et al. provide in this issue’s overview on addiction ( 2 ). The first study in the Blaine et al. article uses 44 patients and 43 control subjects to demonstrate that patients with alcohol use disorder have a blunted neural response to the presentation of stress- and alcohol-related cues. This blunting was observed mainly in the ventromedial prefrontal cortex, a key prefrontal regulatory region, as well as in subcortical regions associated with reward processing, specifically the ventral striatum. Importantly, this finding was replicated in a second study in which 69 patients were studied in relation to their length of abstinence prior to treatment and treatment outcomes. The results demonstrated that individuals with the shortest abstinence times had greater alterations in neural responses to stress and alcohol cues. The authors also found that an individual’s length of abstinence prior to treatment, independent of the number of days of abstinence, was a predictor of relapse and that the magnitude of an individual’s neural alterations predicted the amount of heavy drinking occurring early in treatment. Although relapse is an all too common outcome in patients with substance use disorders, this study highlights an approach that has the potential to refine and develop new treatments that are based on addiction- and abstinence-related brain changes. In her thoughtful editorial, Dr. Edith Sullivan from Stanford University comments on the details of the study, the value of studying patients during early abstinence, and the implications of these findings for new treatment development ( 6 ).
Relatively Low Amounts of Alcohol Intake During Pregnancy Are Associated With Subtle Neurodevelopmental Effects in Preadolescent Offspring
Excessive substance use not only affects the user and their immediate family but also has transgenerational effects that can be mediated in utero. Lees et al. ( 7 ) present data suggesting that even the consumption of relatively low amounts of alcohol by expectant mothers can affect brain development, cognition, and emotion in their offspring. The researchers used data from the Adolescent Brain Cognitive Development Study, a large national community-based study, which allowed them to assess brain structure and function as well as behavioral, cognitive, and psychological outcomes in 9,719 preadolescents. The mothers of 2,518 of the subjects in this study reported some alcohol use during pregnancy, albeit at relatively low levels (0 to 80 drinks throughout pregnancy). Interestingly, and opposite of that expected in relation to data from individuals with fetal alcohol spectrum disorders, increases in brain volume and surface area were found in offspring of mothers who consumed the relatively low amounts of alcohol. Notably, any prenatal alcohol exposure was associated with small but significant increases in psychological problems that included increases in separation anxiety disorder and oppositional defiant disorder. Additionally, a dose-response effect was found for internalizing psychopathology, somatic complaints, and attentional deficits. While subtle, these findings point to neurodevelopmental alterations that may be mediated by even small amounts of prenatal alcohol consumption. Drs. Clare McCormack and Catherine Monk from Columbia University contribute an editorial that provides an in-depth assessment of these findings in relation to other studies, including those assessing severe deficits in individuals with fetal alcohol syndrome ( 8 ). McCormack and Monk emphasize that the behavioral and psychological effects reported in the Lees et al. article would not be clinically meaningful. However, it is feasible that the influences of these low amounts of alcohol could interact with other predisposing factors that might lead to more substantial negative outcomes.
Increased Comorbidity Between Substance Use and Psychiatric Disorders in Sexual Identity Minorities
There is no question that victims of societal marginalization experience disproportionate adversity and stress. Evans-Polce et al. ( 9 ) focus on this concern in relation to individuals who identify as sexual minorities by comparing their incidence of comorbid substance use and psychiatric disorders with that of individuals who identify as heterosexual. By using 2012−2013 data from 36,309 participants in the National Epidemiologic Study on Alcohol and Related Conditions–III, the authors examine the incidence of comorbid alcohol and tobacco use disorders with anxiety, mood disorders, and posttraumatic stress disorder (PTSD). The findings demonstrate increased incidences of substance use and psychiatric disorders in individuals who identified as bisexual or as gay or lesbian compared with those who identified as heterosexual. For example, a fourfold increase in the prevalence of PTSD was found in bisexual individuals compared with heterosexual individuals. In addition, the authors found an increased prevalence of substance use and psychiatric comorbidities in individuals who identified as bisexual and as gay or lesbian compared with individuals who identified as heterosexual. This was most prominent in women who identified as bisexual. For example, of the bisexual women who had an alcohol use disorder, 60.5% also had a psychiatric comorbidity, compared with 44.6% of heterosexual women. Additionally, the amount of reported sexual orientation discrimination and number of lifetime stressful events were associated with a greater likelihood of having comorbid substance use and psychiatric disorders. These findings are important but not surprising, as sexual minority individuals have a history of increased early-life trauma and throughout their lives may experience the painful and unwarranted consequences of bias and denigration. Nonetheless, these findings underscore the strong negative societal impacts experienced by minority groups and should sensitize providers to the additional needs of these individuals.
Trends in Nicotine Use and Dependence From 2001–2002 to 2012–2013
Although considerable efforts over earlier years have curbed the use of tobacco and nicotine, the use of these substances continues to be a significant public health problem. As noted above, individuals with psychiatric disorders are particularly vulnerable. Grant et al. ( 10 ) use data from the National Epidemiologic Survey on Alcohol and Related Conditions collected from a very large cohort to characterize trends in nicotine use and dependence over time. Results from their analysis support the so-called hardening hypothesis, which posits that although intervention-related reductions in nicotine use may have occurred over time, the impact of these interventions is less potent in individuals with more severe addictive behavior (i.e., nicotine dependence). When adjusted for sociodemographic factors, the results demonstrated a small but significant increase in nicotine use from 2001–2002 to 2012–2013. However, a much greater increase in nicotine dependence (46.1% to 52%) was observed over this time frame in individuals who had used nicotine during the preceding 12 months. The increases in nicotine use and dependence were associated with factors related to socioeconomic status, such as lower income and lower educational attainment. The authors interpret these findings as evidence for the hardening hypothesis, suggesting that despite the impression that nicotine use has plateaued, there is a growing number of highly dependent nicotine users who would benefit from nicotine dependence intervention programs. Dr. Kathleen Brady, from the Medical University of South Carolina, provides an editorial ( 11 ) that reviews the consequences of tobacco use and the history of the public measures that were initially taken to combat its use. Importantly, her editorial emphasizes the need to address health care inequity issues that affect individuals of lower socioeconomic status by devoting resources to develop and deploy effective smoking cessation interventions for at-risk and underresourced populations.
Conclusions
Maladaptive substance use and substance use disorders are highly prevalent and are among the most significant public health problems. Substance use is commonly comorbid with psychiatric disorders, and treatment efforts need to concurrently address both. The papers in this issue highlight new findings that are directly relevant to understanding, treating, and developing policies to better serve those afflicted with addictions. While treatments exist, the need for more effective treatments is clear, especially those focused on decreasing relapse rates. The negative affective state, hyperkatifeia, that accompanies longer-term abstinence is an important treatment target that should be emphasized in current practice as well as in new treatment development. In addition to developing a better understanding of the neurobiology of addictions and abstinence, it is necessary to ensure that there is equitable access to currently available treatments and treatment programs. Additional resources must be allocated to this cause. This depends on the recognition that health care inequities and societal barriers are major contributors to the continued high prevalence of substance use disorders, the individual suffering they inflict, and the huge toll that they incur at a societal level.
Disclosures of Editors’ financial relationships appear in the April 2020 issue of the Journal .
1 US Department of Health and Human Services: Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality: National Survey on Drug Use and Health 2018. Rockville, Md, SAMHSA, 2019 ( https://www.samhsa.gov/data/nsduh/reports-detailed-tables-2018-NSDUH ) Google Scholar
2 Koob GF, Powell P, White A : Addiction as a coping response: hyperkatifeia, deaths of despair, and COVID-19 . Am J Psychiatry 2020 ; 177:1031–1037 Link , Google Scholar
3 Cassidy CM, Carpenter KM, Konova AB, et al. : Evidence for dopamine abnormalities in the substantia nigra in cocaine addiction revealed by neuromelanin-sensitive MRI . Am J Psychiatry 2020 ; 177:1038–1047 Link , Google Scholar
4 Bradberry CW : Neuromelanin MRI: dark substance shines a light on dopamine dysfunction and cocaine use (editorial). Am J Psychiatry 2020 ; 177:1019–1021 Abstract , Google Scholar
5 Blaine SK, Wemm S, Fogelman N, et al. : Association of prefrontal-striatal functional pathology with alcohol abstinence days at treatment initiation and heavy drinking after treatment initiation . Am J Psychiatry 2020 ; 177:1048–1059 Link , Google Scholar
6 Sullivan EV : Why timing matters in alcohol use disorder recovery (editorial). Am J Psychiatry 2020 ; 177:1022–1024 Abstract , Google Scholar
7 Lees B, Mewton L, Jacobus J, et al. : Association of prenatal alcohol exposure with psychological, behavioral, and neurodevelopmental outcomes in children from the Adolescent Brain Cognitive Development Study . Am J Psychiatry 2020 ; 177:1060–1072 Link , Google Scholar
8 McCormack C, Monk C : Considering prenatal alcohol exposure in a developmental origins of health and disease framework (editorial). Am J Psychiatry 2020 ; 177:1025–1028 Abstract , Google Scholar
9 Evans-Polce RJ, Kcomt L, Veliz PT, et al. : Alcohol, tobacco, and comorbid psychiatric disorders and associations with sexual identity and stress-related correlates . Am J Psychiatry 2020 ; 177:1073–1081 Abstract , Google Scholar
10 Grant BF, Shmulewitz D, Compton WM : Nicotine use and DSM-IV nicotine dependence in the United States, 2001–2002 and 2012–2013 . Am J Psychiatry 2020 ; 177:1082–1090 Link , Google Scholar
11 Brady KT : Social determinants of health and smoking cessation: a challenge (editorial). Am J Psychiatry 2020 ; 177:1029–1030 Abstract , Google Scholar
- Cited by None

- Substance-Related and Addictive Disorders
- Addiction Psychiatry
- Transgender (LGBT) Issues
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Review Article
- Open access
- Published: 12 August 2021
Drug addiction: from bench to bedside
- Julian Cheron 1 &
- Alban de Kerchove d’Exaerde ORCID: orcid.org/0000-0002-0682-5877 1
Translational Psychiatry volume 11 , Article number: 424 ( 2021 ) Cite this article
16k Accesses
27 Citations
1 Altmetric
Metrics details
- Molecular neuroscience
Drug addiction is responsible for millions of deaths per year around the world. Still, its management as a chronic disease is shadowed by misconceptions from the general public. Indeed, drug consumers are often labelled as “weak”, “immoral” or “depraved”. Consequently, drug addiction is often perceived as an individual problem and not societal. In technical terms, drug addiction is defined as a chronic, relapsing disease resulting from sustained effects of drugs on the brain. Through a better characterisation of the cerebral circuits involved, and the long-term modifications of the brain induced by addictive drugs administrations, first, we might be able to change the way the general public see the patient who is suffering from drug addiction, and second, we might be able to find new treatments to normalise the altered brain homeostasis. In this review, we synthetise the contribution of fundamental research to the understanding drug addiction and its contribution to potential novel therapeutics. Mostly based on drug-induced modifications of synaptic plasticity and epigenetic mechanisms (and their behavioural correlates) and after demonstration of their reversibility, we tried to highlight promising therapeutics. We also underline the specific temporal dynamics and psychosocial aspects of this complex psychiatric disease adding parameters to be considered in clinical trials and paving the way to test new therapeutic venues.
Similar content being viewed by others

Addiction as a brain disease revised: why it still matters, and the need for consilience

The neurobiology of drug addiction: cross-species insights into the dysfunction and recovery of the prefrontal cortex

Mechanisms and molecular targets surrounding the potential therapeutic effects of psychedelics
Introduction.
Drug addiction including smoking, alcohol and illicit drug use is indirectly or directly responsible for 11.8 million deaths each year in the world [ 1 ]. According to the Global Burden of Disease study, this number is higher than deaths from cancer and accounts for a fifth of all deaths around the world [ 1 ].
Drug addiction is defined as a chronic, relapsing disease that results from the prolonged effects of drugs on the brain. Similarly to other neuropsychiatric diseases, drug addiction is intermingled with behavioural and social aspects that are equally important parts of the disease, complicating the overall therapeutic approach. Actually, it is only recently, in the beginning of the 21st century, that we started to see “the drug-addict” as someone suffering from a disease and whose brain has been altered fundamentally by drugs [ 2 ]. Therefore, the most effective treatment approaches include biological, behavioural and social-context components. Based on the latest scientific advances, treatment and management of drug addiction patients point towards a personalised strategy [ 3 ]. However, there are very few objective and effective strategies for treating drug addiction. Without the mandatory mechanistic basic knowledge on drug addiction, the development of new therapeutic strategies is postponed.
The neurobiological circuits and mechanisms that support compulsive seeking and consumption of drugs with addictive potential are partially known. They comprise a progressive shift in the involvement of ventral to dorsal and medial to lateral striatal circuitry [ 4 , 5 ], along with molecular and cellular adaptations to drugs of abuse exposure. They include neuronal and synaptic plasticity and modifications in gene expression, in part through epigenetic mechanisms [ 6 ]. Notably, drug-induced neuronal modifications can also occur in non-pathological processes, underlying the fact that drugs of abuse hijack normal adaptive changes in the brain [ 7 ]. Indeed, laboratory and clinical observations suggest that addiction is driven by the usurpation of neuronal processes that normally serve reward-related learning and memory. Most of the modifications that have been shown to be involved in a state of addiction (modified gene transcription, epigenetics, neuronal plasticity and neurotrophic mechanisms) are also associated with physiological forms of behavioural memory in murine model such as spatial memory, fear conditioning and operant conditioning [ 7 , 8 ].
We know that only a proportion of individuals (depending of the drug type) will develop drug addiction after several exposures [ 9 ]. This individual vulnerability is probably linked to both genetic and environmental factors [ 10 ]. Drug addiction is highly polygenic, as hundreds of genetic variations combined result in variable vulnerability [ 11 , 12 ]. Several types of environmental factors have been characterised and interact with an individual genetic background [ 12 , 13 ]. Psychosocial stress is one of the factors, but the most important one, is by far, the exposure to drugs of abuse. Usually, drug abuse starts with a ‘gateway’ drug (mostly socially driven) catapulting the individual vulnerability to other drugs of abuse [ 14 ].
During the last three decades, combine effort has been dedicated to identify brain regions and molecular pathways involved in the development of addiction to drugs of abuse. Here, we will focus on experimental approaches that helped to provide a clearer picture on the physiopathology of drug addiction guiding therapeutic opportunities.
Converging actions on brain reward pathway elicit its remodelling
The circuit at the centre of the disease is the mesolimbic pathway, also referred as the reward pathway (Fig. 1 ). The mesolimbic pathway includes dopaminergic neurons in the ventral tegmental area (VTA) of the midbrain and their targets in the limbic forebrain, especially the nucleus accumbens (NAc), a major component of the ventral striatum. The GABA medium-sized spiny neurons (MSNs, ~95% of striatal neurons), which are targets of glutamatergic and dopaminergic inputs, form two pathways [ 15 ]. The dopamine D1 receptor–positive (D1R) striatonigral MSNs project to the medial globus pallidus and substantia nigra pars reticulata (direct pathway) and coexpress dopamine D1 receptors and substance P, whereas D2R striatopallidal MSNs project to the lateral globus pallidus (indirect pathway) and coexpress dopamine D2 receptor, adenosine A2A receptor and enkephalin [ 16 , 17 ]. Through different initial mechanisms, drugs of abuse increase the release of dopamine in the NAc from the VTA [ 18 , 19 , 20 ]. This VTA-NAc pathway could be seen as primum movens for the acute rewarding effects of all drugs of abuse. Regardless that drugs of abuse have distinct protein targets and mechanisms of action, in the end, the main addiction-related modifications are common to nearly all drugs of abuse and converge on the VTA and NAc with common acute functional effects [ 21 ]. It is schematically conjectured, that when stimulated by dopamine, cells in the NAc produce feelings of reward and satisfaction [ 22 ]. The physiological function of this response is to facilitate the motivation for basic biological goal-directed behaviours as survival, social interaction and reproduction. By artificially causing a build-up of dopamine in the NAc, drugs of abuse generate an artificial reward effect [ 22 ]. As all drugs of abuse increase dopaminergic transmission to the NAc after acute administration, they also produce shared modifications in the mesolimbic system after chronic exposure. They include (i) hypofunction of the dopamine pathway that is seen as a major contributor to the negative emotional symptoms associated to drug withdrawal, leading to drug craving and relapse, and (ii) drug-induced adaptations in glutamatergic afferents to the NAc [ 23 , 24 ]. Clearly, these modifications in the mesolimbic system after the exposure to drugs of abuse is oversimplified. The hypofunction of dopaminergic system hypothesis is self-fulfilling in that research work has principally focused on dopamine to the exclusion of other neurotransmitters. Actually, some drug of abuse reinforcement appears to be independent of the mesocorticolimbic dopamine system (e.g. opioids [ 25 ], nicotine [ 26 ]), but support self-administration by imitating the effect of dopamine in the nucleus accumbens [ 21 , 27 , 28 ].

Addictive drugs of different types have a common effect of increasing levels of dopamine released by neurons projecting from the ventral tegmental area (VTA). This effect is central for initial drug reinforcement. Notably, drug taking with initial reinforcement involves a potentiation of the projection from prefrontal cortex (PFC) to nucleus accumbens (NAc), while other glutamatergic projections are mostly involved in craving, like basolateral amygdala (BLA)-NAc projection, or in withdrawal/negative symptoms, like paraventricular thalamus (PVT)-NAc projection. With increasing administration of drugs of abuse and progressive shift toward compulsive abuse, the dorsal (dorso-lateral) striatum seems more and more implicated, with dopaminergic cells involved shifting progressively from the VTA to the substantia nigra pars compacta (SNc) [ 4 ]. Recently, data acquired through optogenetic dopamine neuron self-stimulation suggested prominent synaptic strengthening of the orbitofrontal cortex (OFC) to dorsal (dorso-medial) striatum projection in compulsive mice [ 31 ].
Drug addiction is conceptually defined as a three-stages cycle: (1) consumption/binge/intoxication, (2) withdrawal with its negative affect and (3) craving stage (Fig. 2 ) [ 27 ]. Animal models and human imaging studies have exposed the different brain areas involved in each of these stages. Briefly, the VTA-NAc (for reinforcement) and dorsal striatum (for stimulus-response habits) are important for the consumption/binge/intoxication stage, the extended amygdala with the hypothalamus and the brainstem in the withdrawal stage and cortical areas, the dorsal striatum, the hippocampus and the basolateral amygdala in the craving stage (Fig. 2 ).

Progression to addiction is defined as a transition between three consecutive phases [ 252 ]: (1) Recreational, sporadic drug taking, in which drug of abuse administration is occasional and one activity among many other distractions of the individual. (2) Intensified and sustained drug use, in which drug administration strengthens and becomes the principal recreational activity of the individual; at this phase drug taking becomes a habit. (3) Loss of control of drug use and addiction, in which drug seeking and taking are now the principal activity of the patient. The first phase can occur to every person as drugs of abuse hijack the same brain circuit as natural rewards. The second phase occurs only in vulnerable users. The phase of addiction seems to be due to a second vulnerable trait with loss of control and compulsivity. Three stages of addiction are described [ 27 ]: (1) Binge/intoxication stage: reinforcing effects of drugs may initially use mainly dopamine and opioid peptides in the nucleus accumbens (NAc) and involves the ventral tegmental area (VTA). Subsequently, cue–response habits develop and includes the substantia nigra pars compacta (SNc) and the dorsal striatum. (2) Withdrawal/negative affect stage: the negative emotional state of withdrawal may involve the extended amygdala with corticotropin-releasing factor (CRF), norepinephrine and dynorphin as key neurotransmitters. Main projections of the extended amygdala consist of the hypothalamus and brainstem. (3) Craving stage: this stage includes conditioned reinforcement in the basolateral amygdala (BLA) and contextual processes in the hippocampus. This is controlled by cortical areas (prefrontal cortex (PFC) and orbitofrontal cortex (OFC)). A key neurotransmitter involved in the craving stage is glutamate.
The progression of drug addiction begins with the first exposure, mostly when the drug is taken voluntarily for its recreational and hedonic effect, and progressively consolidates during repeated but still controlled drug use. While administration intensifies along with loss of control over drug intake, drug use becomes habitual and compulsive in vulnerable individuals [ 4 , 29 , 30 ] (Fig. 2 ). This progression from voluntary drug intake to habitual and compulsive use represents a progression from ventromedial to more dorsolateral regions of the striatum and from prefrontal cortex (PFC) to orbitofrontal (OFC) and more global cortical region [ 4 , 31 ] (Fig. 1 ).
Synaptic plasticity
Brain plasticity is a fascinating capacity allowing appropriate modification of the neural activity in response to new experiences and environmental stimuli [ 32 ]. Modifying the synaptic strength between neurons is widely assumed to be the mechanism by which memory is encoded and stored in the brain [ 7 ]. Hence, it is appealing to hypothesise that drugs of abuse cause long-term alterations on behaviour by changing synaptic plasticity in key brain circuits [ 4 , 7 , 32 ].
Drugs of abuse such as cocaine induce specific synaptic plasticity in the mesolimbic circuitry. One single injection of an addictive drug can already modify the excitatory synaptic strengths in the VTA. Indeed, it has been extensively shown that the AMPA/NMDA ratio is increased in VTA dopamine neurons after one dose of cocaine and that some glutamate AMPA receptor 2 (GluA2)-containing AMPA receptors (AMPARs) are exchanged for GluA2-lacking ones [ 33 , 34 ]. At the same time, NMDA receptor (NMDAR) function decreases. All these elements cause an impairment in eliciting long-term potentiation (LTP). Different types of synaptic plasticity in VTA dopamine neurons induced by rewarding and aversive experiences are comprehensively reviewed by Pignatelli and Bonci [ 35 ]. Midbrain dopamine neurons are central in the mesolimbic circuitry for both natural rewards and drugs of abuse [ 18 , 36 ]. The VTA is known to be a central hub integrating numerous inhibitory inputs as GABAergic synapses represents 50–80% of all synapses onto VTA dopamine neurons [ 37 , 38 , 39 ]. GABAergic inhibition of dopamine neurons is mediated by both fast ionotropic GABA A receptors and slow metabotropic GABA B receptors [ 40 ].
In 2017, Edwards et al. [ 41 ] showed that the principal monosynaptic projection to VTA dopamine neurons arising from the NAc [ 42 ] inhibits the firing of dopamine neurons via activation of GABA B receptors, whereas local VTA inhibitory interneurons inhibits dopamine neurons through GABA A receptors. Today, it is well established that pharmacological activation of GABA B receptors (e.g. by baclofen) reduces cue-associated cocaine craving as well as reduce cocaine use in humans [ 43 , 44 , 45 ] and it reduces rewarding and reinforcing effects of cocaine on animal models [ 46 , 47 , 48 , 49 ]. Edwards et al. report [ 41 ] indicates that the therapeutic effects of baclofen might pass through VTA dopamine neurons’ GABA B receptors. Intrathecal Baclofen is an effective and safe long-term treatment used worldwide to treat severe spasticity [ 50 , 51 ]. Oral baclofen is less effective and has significant rates of side effects, like sedation, somnolence, vertigo and headache especially when prescribed off-label for drug addiction (because higher doses are commonly used) [ 51 , 52 ] . . Indeed, contrasting results on the effect of baclofen in reducing alcohol craving [ 53 , 54 , 55 ] and cocaine dependence [ 43 , 56 ] were probably due to different severity of alcohol dependence of the enroled patients. This is way higher dose are tested and often prescribed off-label for drug addiction [ 55 ]. Thus, self-poisoning that could lead to severe toxicity and death represents one the major concern of baclofen use in drug addiction. Therefore, baclofen should be prescribed with caution and close monitoring [ 52 , 57 ].
Together with drug of abuse-induced LTP at excitatory synapses, plasticity of GABAergic inhibitory synapse in the VTA also have an impact on the firing rate of VTA neurons, at least following opioid [ 58 ] and cocaine administration [ 59 ]. Normally, NMDA activation, during excitatory LTP (induced by high-frequency stimulation), leads to the release of NO that will activate guanylate cyclase in adjacent GABAergic terminals, which in turn, leads to increase in GABA release. This presynaptic NMDA receptor-dependent GABAergic LTP heterosynaptic plasticity, is named LTP GABA . Nugent el al. [ 58 ] showed that opioids blocks LTP GABA through a disruption of the coupling between nitric oxide (NO) and guanylate cyclase. The incapability of GABAergic synapses to potentiate after morphine or cocaine administration may promote LTP of glutamatergic synapses [ 58 , 59 ]. The early loss of inhibitory control combined with potentiation of glutamatergic synapses on dopaminergic neurons might represent adaptations that increase vulnerability to addiction [ 58 , 59 ]. Furthermore, GABA A receptor modulators modify the addictive drugs effects [ 60 , 61 ], and targeting these receptors might be seen as an effective therapeutic strategy but precluded by many side effects among which dependence itself [ 62 , 63 , 64 ].
In addition to the discovery of LTP GABA , Nugent’s group showed that morphine is also able to modulate a form of postsynaptic LTD (LTD GABA ) at GABAergic synapses onto VTA dopamine neurons. Remarkably, after a single administration of morphine, LTD GABA was absent in slices from morphine-treated rats while unaffected in slices from saline-treated rats, indicating a bidirectional control of morphine on GABAergic synaptic plasticity in the VTA [ 65 ]. This absence of LTD GABA is suggested to result from an occlusion effect due to prior morphine-induced decrease in GABAergic synaptic strength through potentiation of glutamatergic transmission and mediated by endocannabinoid signalling [ 66 ]. It is also possible that morphine alters the ability of synapses to exhibit evoked LTP or LTD in the VTA. Previous experiences such as exposure to drugs of abuse, stress, visual or sensory deprivation can change the ability of synapses to undergo subsequent plasticity in response to LTP and LTD induction protocols. This concept of modification of plasticity capability is referred as metaplasticity [ 67 ].
In the NAc, chronic exposure to addictive drugs induces specific synaptic changes that are different from those of the VTA, including a decrease of the AMPA/NMDA ratio as some AMPARs are endocytosed. This leads to a depressed synapse (sometimes referred as long-term depression (LTD) like state), where NMDAR-dependent LTD is reduced or, in some experiments, abolished [ 68 , 69 ]. Highlighting the importance of temporal aspects, studies of withdrawal period after chronic administration of cocaine, showed that synaptic AMPAR levels increase during the first week of withdrawal and persist elevated for weeks [ 70 , 71 , 72 ]. It is established that cocaine challenge transiently decreases AMPAR surface expression, while AMPARs recover back to upregulated levels within a week, with a continuous increase during what is known to be the incubation of craving stage [ 73 ].
The abstinence period after withdrawal is of particular interest considering the classical progression of the disease, the chance of relapse and the opportunity for new therapeutic targets. A seemingly counterintuitive concept named ‘incubation of cocaine craving’ was introduced by Grimm et al. [ 74 ] who modelled cocaine-craving behaviour by using rats trained to press a lever to receive an injection of cocaine and were then forced in a withdrawal period where cocaine reward was no longer given. This concept of ‘incubation’ did not originate in drug addiction research but came from a four-stage model of the creative process proposed by Graham Wallas in 1926 [ 75 ]. Consistent with clinical observations in humans [ 76 , 77 , 78 ], they showed that relapse was progressively stronger over 2 months of cocaine withdrawal and suggest that a craving syndrome progresses or ‘incubates’ during the first 2 months of cocaine abstinence, and probably lasts for longer [ 74 ]. Subsequently, it was shown that this increase was due to the addition of new AMPARs lacking GluA2 and that these new receptors mediate the ‘incubation of cocaine craving’ [ 72 ]. Conrad et al. [ 72 ] showed that after extended withdrawal from cocaine, addition of synaptic AMPARs together with the increased conductance of GluA2-lacking AMPARs triggers higher sensitivity of NAc neurons to cocaine-related cues, leading to a strengthening of drug craving syndrome and relapse. In line with these results, it was suggested that as soon as abstinence is reached, the risk of relapse might be reduced if GluA2-lacking AMPARs were inactivated or removed from NAc synapses. It was thus proposed that GluA2-lacking AMPARs could be a new target for drug development for the treatment of cocaine addiction. While these calcium permeable AMPARs are also critical for the pathogenesis of numerous other neurological disorders (including epilepsy [ 79 ], fragile X syndrome [ 80 ], amyotrophic lateral sclerosis [ 81 ], Parkinson’s [ 82 ] and Alzheimer’s [ 83 ] diseases), developing drugs that specifically target them and not calcium-impermeable AMPARs, which are critical for normal CNS function, is challenging [ 84 ] (Fig. 3 ).

DNA is packaged inside nuclei with the help of histones. These are positively charged proteins that strongly adhere to negatively charged DNA and form complexes called nucleosomes. Each nucleosome is composed of DNA wound around histone octomers (H2A, H2B, H3 and H4). Nucleosomes fold up to form chromatin fibre, which forms loops compressed and folded to produce fibres, which are coiled into the chromatid of a chromosome. Only by loosening compacted chromatin, the DNA of a specific gene can be made accessible to transcription. Some of these drug-induced modifications at the chromatin level are extremely stable and sustain the drug of abuse-induced long-term behaviours. Among them, histone post-translational modifications (PTMs) are known to be causally involved in drug-induced behaviours [ 194 ]. PTMs include acetylation (Ac), methylation (Me), phosphorylation (P), ADP ribosylation (PolyADP-R) and dopaminylation (DA), among a growing list of newly discovered modifications [ 162 , 172 ]. For example, while ubiquitylation (Ub) of H2A is known to be a key interactor of H3 methylation [ 253 ], its supposed role in drug addiction is still unknown. At this epigenetic level, some drugs were demonstrated to have an influence on drug-induces behaviours such as histone deacetylase (HDAC), bromodomain and DNA methyltransferase inhibitors. Locus-specific epigenome editing is now encouraging as a new field of investigation as it might help to the discovery of new specific and causal drug of abuse targets. Overview of the tetrapartite glutamatergic synapse composed of a medium spiny neuron (MSN), a glutamatergic projection, a glial cell and the extracellular matrix (ECM). Here, we focused on synaptic potentiation after drug of abuse administration with the addition at the post-synaptic membrane of glutamate AMPA receptor 2 (GluA2) lacking AMPA receptors (AMPARs). This mechanism might be reduced by metabotropic glutamate receptor 1 (mGluR1) positive allosteric modulator or more directly by GluA2-lacking AMPARs antagonists. In the same way, it was also shown that presynaptic mGluR2 agonists can potentially abolish drug seeking and impair craving incubation. Optogenetically-inspired 12 Hz deep brain stimulation (DBS) in the nucleus accumbens can also be a promising novel therapeutic for addiction. Finally, ceftriaxone, N-acetylcysteine, and inhibitor of matrix metalloproteases 9 (MMP-9), mainly through their action on glial cell and the ECM, are very interesting molecules that may be added in the addiction therapeutic arsenal.
Inspired by previous work performed in the VTA showing that metabotropic glutamate receptor 1 (mGluR1) LTD induces removal of GluA2-lacking AMPARs from synapses [ 33 , 34 ], Loweth et al. [ 85 ] demonstrated that synaptic GluA2-lacking AMPAR decrease could be accomplished by in vivo evoked mGluR1 LTD in the NAc. More importantly, their group showed that after prolonged cocaine or methamphetamine withdrawal, systemic injection of a mGluR1 positive allosteric modulator attenuated the expression of incubated craving by reducing GluA2-lacking AMPARs in the NAc [ 85 , 86 ]. These results suggest a strategy in which abstinent methamphetamine or cocaine users could use a systemically active compound to protect themselves against cue-induced relapse.
These latter studies were conducted without differentiating between D1 receptor D1R MSNs and D2R MSNs. In 2014, Pascoli et al. [ 87 ] demonstrated that this increase in the strength of excitatory afferents was exclusively related to D1R MSNs. Interestingly, the type of drug-evoked plasticity involved is also dependent on the input. It has been shown that even in the same D1R MSN a synapse connecting the PFC to the NAc increases its strength by inserting GluA2-lacking AMPARs whereas a synapse connecting the ventral hippocampus to the NAc increases the AMPA/NMDA ratio by inserting GluA2-containing AMPARs [ 87 ].
Besides operant self-administration, all these long-term synaptic modifications also underlie behavioural changes associated with drugs of abuse, such as locomotor sensitisation [ 88 , 89 ]. Locomotor sensitisation is a behavioural protocol used to model drug-induced behaviour [ 90 , 91 ]. In rodents, repeated cocaine injection induces gradually increased locomotor activity; after 5 days of consecutive injections, the locomotor response reaches a ceiling level. This state lasts for months after cocaine withdrawal [ 91 ]. As an experimental model, locomotor sensitisation is linked with increased tendency to self-administer psychostimulants [ 92 , 93 ] and with reinstatement of previously extinguished self-administration [ 94 , 95 ]. Whereas the existence of psychomotor sensitisation in humans is discussed [ 96 , 97 ], it is a key aspect of vulnerability to drug addiction and relapse, specifically drug craving or compulsive drug-seeking behaviour [ 91 , 98 , 99 ]. Still, locomotor sensitisation can be dissociated from the rewarding effect of a drug of abuse and conditioned place preference or self-administration are more appropriate experimental paradigms to test this aspect [ 100 , 101 , 102 ]. Even if drug-induced locomotor sensitisation is unclearly present in humans, as an animal model it offers a clear readout to understand the mechanisms by which drugs of abuse induce long-term brain modifications [ 91 ].
Furthermore, it has been elegantly demonstrated that optogenetic stimulation of the excitatory projections to the NAc is able to reverse cocaine and alcohol-evoked plasticity [ 87 , 88 , 89 ]. Briefly, applying a NMDAR or mGluR1-dependent LTD on cortico-accumbal glutamatergic synapses, before a drug of abuse administration, diminishes its effect. In another study, Luscher’s team took advantage of the knowledge, obtained from optogenetic in vivo experiment in rodents, to implement a novel deep brain stimulation (DBS) protocol that abolishes behavioural sensitization to cocaine (and thus that would be efficient during the relapse phase) [ 103 ]. Basically, the idea is to manipulate synaptic plasticity in the NAc to reverse pathological synaptic transmission and its associated behaviours following exposure to drugs of abuse. In this study, as a therapeutic use of optogenetic tools in humans is for now inapplicable [ 104 ], the authors reversed cocaine-evoked plasticity and thus drug-induced behaviours by using DBS instead of optogenetic. Indeed, DBS is routinely used in clinic and a new DBS protocol can easily be translationally implemented to the human therapeutics [ 105 , 106 ]. They refined the classical high-frequency DBS protocol (that has no sustained effect on cocaine sensitization, probably because it does not affect synaptic plasticity) by applying a low frequency stimulation (12 Hz to equal the one used in the optogenetic endocannabinoid- dependent LTD protocol) in the NAc together with the administration of a D1R antagonist necessary to unmask the mGluR-dependent LTD in D1R MSNs as demonstrated previously [ 107 ] (Fig. 3 , see section on clinical treatment for broader discussion on DBS).
Kalivas’ group showed in 2009 [ 108 ] that after extended withdrawal from chronic cocaine self-administration, cocaine-induced metaplasticity at the excitatory synapses in the NAc that impairs the ability of PFC stimulation to produce LTP or LTD in NAc MSNs. They also showed that N-acetylcysteine reverses cocaine-induced metaplasticity, allowing the induction of both LTP and LTD and that N-acetylcysteine decreases cocaine-relapse in a rodent model. We are currently awaiting the results of a randomised and control study that is testing newly detoxified (and therefore abstinent) hospitalised patients who received a 3–4 week course of treatment, in order determine if N-acetylcysteine can be a useful medication candidate to avoid relapse in patients with cocaine dependence (NCT03423667).
GABAergic D1R and D2R MSNs, equally compose and are mosaically intermingled throughout the striatum [ 109 ]. As explained above, D1R and D2R MSNs send axonal projections outside the striatum, forming the two main output pathways, respectively the direct and indirect pathways [ 16 , 17 ]. In a certainly oversimplified model, the activation of the D1R MSNs result in facilitation of locomotion, reward, and reinforcement while the activation of D2R MSNs result in opposing effects [ 110 , 111 , 112 , 113 ]. In addition to the long-range projections, these neurons form short-range synaptic connections with one another within the striatum, and because they consist of inhibitory collaterals, a mechanism known as lateral inhibition [ 114 , 115 , 116 , 117 ]. Interestingly, these connections are not symmetrical, with D2R MSNs forming more synaptic connections on D1R MSNs [ 115 , 117 ]. Through this previously understudied collateral transmission, Dobbs et al. [ 115 ] presented a novel mechanism by which cocaine exerts its stimulant effect: cocaine, by blocking DAT receptors enhance levels of dopamine and subsequently activating D2Rs, causes a suppression of lateral inhibition and thus disinhibition of D1R MSNs in the NAc which in turn promotes locomotion [ 115 ]. Furthermore, Alvarez’ group suggested that constitutive low D2R levels, through imbalanced lateral inhibition, might pre-sensitised D1R MSNs, facilitate behavioural plasticity to repeated cocaine and promotes an addiction vulnerable phenotype [ 116 ].
The characterisation of the role of glia and the extracellular matrix (ECM) in drug-induced synaptic plasticity is an exciting emerging field of drug addiction research as it comes with promising new therapeutic possibilitiess [ 118 , 119 , 120 ]. Mulholland et al. [ 118 ] summarised and emphasised the role of the ECM and of astroglial cells in the regulation of synaptic plasticity. Of great interest, restoring downregulated glutamate transporter 1 (EAAT2) with ceftriaxone reduces drug seeking in animal models [ 121 , 122 ]. Matrix metalloproteases (MMP) are important regulators of the ECM and contribute to synaptic plasticity [ 123 ]. Inhibiting their activity result in suppression of the reinstatement of cocaine conditioned place preference [ 124 ] and selectively inhibiting MMP-9 prevents cue- and cocaine-induced reinstatement of cocaine self-administration [ 119 ]; these results open additional therapeutic possibilities with the use of inhibitors of MMP-9 as an innovative targeted approach [ 119 , 124 , 125 ] (Fig. 3 ). Still, at our knowledge, there are no randomised controlled study currently investigating these ECM-related drugs.
Drugs of abuse-induced modifications in glutamatergic nuclei targeting the NAc, or the VTA and essential part of the reward circuit, are less studied than cortico-striatal synapses despite the fact that they play a crucial role in the development of drug addiction. Indeed, in the OFC and PFC, chronic alcohol exposure significantly increases LTP in pyramidal neurons [ 126 , 127 ]. Kazanetz et al. [ 128 ] showed that repeated cocaine injections impair endocannabinoid-LTD and mGluR2/3-LTD in the PFC. They postulated that this might mechanistically participate in the induction of a postsynaptic, observed LTP-like phenomenon with an enhanced AMPA/NMDA ratio. It was also demonstrated that neurons of the infralimbic cortex present a decrease in mGluR2 [ 129 ]. In addition, alcohol-dependent rats exhibit an escalation of ethanol seeking, which was abolished by restoring mGluR2 expression in the infralimbic cortex via viral-mediated gene transfer [ 129 ]. Notably, mGluR2 agonist was shown to impair the incubation of cocaine craving [ 130 ] and to attenuate reinstatement of cocaine-seeking [ 131 , 132 ](Fig. 3 ). Recently, Caprioli et al. [ 133 ] extensively reviewed preclinical studies on allosteric modulators of mGluRs on animal models of drug addiction and their potential translational implications. The results reviewed [ 133 ] indicate an remarkable effect of allosteric modulators of presynaptic mGluR2 and possibly mGluR7, supporting the idea that these compounds should be tested as potential medications for addiction treatments.
Besides the PFC, other brain regions appear to be key areas in drug addiction as the paraventricular thalamus (PVT) - a central hub for cortical, sensory and limbic information [ 134 , 135 , 136 , 137 , 138 , 139 , 140 ]. In 2016, Zhu et al. [ 141 ] showed that chronic morphine administration potentiates excitatory synapses between the PVT and D2R MSNs via insertion of GluA2-lacking AMPARs. Remarkably, in vivo optogenetic depotentiation at these synapses abolishes morphine withdrawal symptoms. In a recent paper, projections from the PVT to the NAc were shown to be critical for augmentation of heroin seeking in food-restricted rats [ 142 ] (Fig. 1 ). Actually, Otis et al. [ 143 ] demonstrated that the PVT is an integrative hub for reward seeking behaviour and that PVT-NAc neurons integrate different inputs from the PFC and the lateral hypothalamus to precisely guide reward seeking behaviour. In a recent review, De Groote et al. [ 140 ] focused on the new advances in the understanding of the roles of the PVT-NAc connections in motivated behaviours, highlighting their implications in drug addiction.
Drug addiction-related genes and transcriptomic regulation
Modifications in gene expression contribute to the long-lasting effect sustaining drug addiction; thanks to gene-expression arrays, RNA-sequencing and candidate gene approaches, the specific genes and their regulatory transcriptomic mechanisms involved in drug addiction development and maintenance are now better understood.
Drug addiction-related genes
For example, the use of conditional gene knockout in mice emphasises the importance of monoamine membrane transporters (dopamine transporter, and serotonin transporter) [ 144 , 145 ] and of mGluRs [ 146 , 147 ]. As new animal models of drug addiction, these approaches are also useful to better characterise fine-tuning of important pathways involved in addiction. For example, a scaffold protein known as Maged1 has been shown to be involved in cocaine reward and reinforcement [ 148 ]. We demonstrated that Maged1 inactivation impairs drug-evoked dopamine release and glutamatergic synaptic plasticity in the NAc. Inactivation of Maged1 in mice was able to abolish behavioural sensitization to cocaine as well as cocaine conditioned place preference and operant self-administration behaviours [ 148 ]. This sole genetic alteration, causally linked to a strong alteration of drug-induced behaviours, impairs (at least) two core neuronal mechanisms leading to addictive behaviours: (1) cocaine-evoked release of dopamine in the NAc and (2) NAc plasticity, with a reduced AMPA/NMDA ratio and a resistance to LTD. Actually, it seems that, after Maged1 inactivation, the excitatory synapses in the NAc shift to a depressed state. Our hypothesis is that, in line with the previously discussed in vivo optogenetic induced LTD, this impairment could be a key factor for the significant decrease in sensitization to psychostimulants [ 87 , 103 , 148 ]. Actually, it seems that placing neurons in a state of ‘presensitization’ is able to prevent drug-induced sensitization itself [ 148 , 149 ]. Our group is now trying to understand what are the cellular and molecular pathways directly altered by Maged1 inactivation and responsible for this strong anti-addictive drug phenotype. Remarkably, the promoter of Maged1 was found in a list of 213 promoters that co-precipitate with acetylated histones and with the activated form of cAMP response element binding protein (CREB) after chronic drug taking [ 150 ]. In line with this result, preliminary and unpublished results from our laboratory point out a specific epigenetic mechanism, in parallel with an alteration of synaptic plasticity in excitatory projection to the NAc, that would link Maged1 to its major effect on drug-induced behaviours. This selected gene approach is of great interest in refining our knowledge of pathways hijacked by addictive drugs. Using cell sorting of D1R MSNs and D2R MSNs as described previously [ 151 ], our group also identified the G-protein-regulated inducer of neurite outgrowth 3 (GPRIN3) in both MSN populations but strikingly more expressed in D2R MSNs [ 149 ]. The GPRIN family (GPRIN1, GPRIN2 and GPRIN3) are Gαi/o-regulated proteins suggested to intermediate the communication between GPCRs and the sequential intracellular target [ 152 ]. Indeed, GPRIN1 and GPRIN2 have been described as alternative (to adenylyl cyclase) mediators of GPCRs signalling but GPRIN3 had a much less defined role [ 152 , 153 ]. To understand the role of GPRIN3 in the pathophysiology of the D2R-indirect pathway, we induced a D2R-MSNs-specific knockdown (KD) of GPRIN3 using small hairpin RNA and lentiviruses [ 151 , 154 ]. We first observed a significant increase in distal branching, the points of convergence between glutamate and dopamine synapses in MSNs [ 155 ] and also key targets of cocaine, which itself promotes increase in distal branching in the NAc of mice [ 156 , 157 , 158 , 159 ]. Thus, we tested the cocaine acute effect and locomotor sensitization and observed a decrease in cocaine-induced hyperlocomotion after inactivation of GPRIN3 using a CRISP/Cas9 approach. The significant increase in distal branching in GPRIN3 D2R-MSNs KD corroborates our hypothesis that the lack of GPRIN3 induces a ‘presensitization process’, able to change the targets of cocaine and therefore altering its effects [ 149 ]. Finally, we provide the first evidence that GPRIN3 partners with D2R in the striatum and modulates cocaine-induced behaviours [ 149 ].
Transcriptomic and epigenetic regulations
Epigenetics is a broad field and has multiple definitions that comprise several biochemical mechanisms (including DNA methylation and histone modifications) sustaining modifications in gene expression throughout the lifecycle of an organism without mutations of the DNA itself [ 160 , 161 , 162 ]. Epigenetics can be considered as the process through which environment (and normal development) interacts with an individual’s genome to determine all phenotypic traits, in health and disease. Stable modifications in gene expression are also said to be ‘epigenetic’, because they are heritable in the short term (through mitosis) [ 160 ] and in some cases trans-generationally, thus, providing a potential mechanism for environmental influences to be passed from parents to offspring [ 163 , 164 , 165 ]. Handel and Romagopalan [ 163 ] mentioned that “epigenetics allows the peaceful co-existence of Darwinian and Lamarckian evolution”. Such trans-generational epigenetic inheritance of drug addiction vulnerability remains debatable [ 161 ], but has been increasingly studied for the last 20 years [ 166 , 167 ]. Some epigenetic changes are very stable, an thus mediate both drug addiction susceptibility and drug-induced brain alterations that underlie the development of drug addiction [ 161 ].
As the NAc is seen as the central hub of drug addiction, with the notion that chronic drug use induces long-lasting structural, electrophysiological and transcriptional changes in the NAc, researchers are mostly targeting epigenetic modifications in NAc cells. Still, considering initial reports of cocaine-induced epigenetic modifications [ 168 , 169 ], it might be relevant to study further epigenetic changes in other regions such as glutamatergic inputs to the NAc, and further in the VTA, as they are implicated in the physiopathology of drug addiction [ 170 , 171 ] as mentioned above.
To date, the three main epigenetic mechanisms consist of (1) DNA methylation, (2) action of the non-coding RNAs and (3) histone post-translational modifications (PTMs). As an illustrative example, we will focus here only on histone PTMs. PTMs of histone residues on their N-terminal tails, that protrude from the nucleosome core, control chromatin condensation and the switch between euchromatin and heterochromatin and thus DNA-accessibility and gene expressions. PTMs include acetylation, methylation, phosphorylation, ADP ribosylation, ubiquitylation and sumoylation, among a growing list of newly discovered modifications [ 162 , 172 ].
Among these PTMs, the most studied is the acetylation of H3 and H4, that is increased in the NAc after chronic exposure to drugs of abuse [ 150 , 173 , 174 ]. This increase in global acetylation levels is the result of drug-induced alterations in the balance of histone acetyltransferase and histone deacetylase (HDAC) function and is associated with gene activation. CREB-binding protein, a histone acetyltransferase critical to memory processes [ 175 ], is required for cocaine-induced increases in histone acetylation in the NAc [ 176 ].
Fifteen years ago, Tsankova et al. [ 177 ] showed that imipramine, a monoamine reuptake inhibitor used for decades to treat depression, was effective through histone remodelling in depression and highlight the therapeutic potential for chromatin regulation with histone methylation and deacetylation inhibitors in depression. Nevertheless, like with synaptic plasticity (see above), discovering a drug that would interfere with epigenetic mechanisms and thus decrease drugs of abuse effect faces temporal aspects issues [ 173 , 176 , 178 , 179 , 180 , 181 , 182 ]. Indeed, timing has a strong impact considering conflicting results obtained after experimental manipulations of histone acetylation. An acute administration of HDAC inhibitors systemically or directly into the NAc, promotes behavioural responses to the drugs. However, prolonged administration decreases cocaine behavioural effects. In 2013, adding a new layer of complexity, Kennedy et al. provided comprehension to this time-dependent regulation [ 183 ]. Remarkably, they showed that prolonged intraNAc administration (but not acute administration) of a HDAC inhibitor attenuated cocaine behavioural effects by inducing a form of repressive histone methylation. This study showed, for the first time, cross-talk among different types of histone modifications [ 183 ]. Besides cross-talk between different epigenetic modifications, multiple modifications work in parallel and there is often a decoupling between an observed modification at a specific locus and its final transcription [ 161 ]. Decoding these chromatin marks will be a future challenging field. Like with HDAC inhibitors, there are promising findings based on the use of DNA methyltransferases inhibitor [ 184 , 185 ] (Fig. 3 ). Though, the main issue with these new potential treatments for drug addiction is their lack of specificity. One of the key challenge for the pharmaceutical industry will be to generate small molecules with more specific targets [ 6 ].
While histone acetylation and methylation are increasingly studied, an important field of future investigation will be to understand the other drug-induced histone PTMs. It already seems that chronic cocaine alters levels of histone phosphorylation [ 174 , 186 , 187 ], and poly-ADP ribosylation [ 188 ]. Recently, an unexpected role for the intracellular dopamine in VTA has been revealed, showing that DA interacts with chromatin to initiate a new form of epigenetic regulation called dopaminylation [ 189 ] (see Table 1 for a summary of cocaine-related epigenetic modifications).
Further studies showed that histone PTMs that occur in the NAc after chronic drug administration are locus specific [ 150 , 190 , 191 ]. Even though, drugs of abuse alter global levels of multiple histone PTMs, such as increased histone acetylation or decreased methylation in the NAc, genome-wide studies have confirmed that a greater number of genomic sites show increased acetylation [ 150 ] or decreased methylation [ 190 , 191 ]. Conversely, hundreds of genes show opposite or no changes in these same PTMs after drug exposure. What defines whether, and in which direction, a specific gene is modified in the context of a global histone PTM is an intriguing and unsolved question [ 161 ]. These genome-wide studies (ChIp on chip or ChIpSeq) are nowadays fundamental to understand where PTMs and other epigenetic modifications are deposited. This will be fundamental to guide new therapeutics.
Actually, with new tools such as zinc finger proteins (ZFPs) DNA-binding domains and, more recently, RNA-guided CRISPR/dCas9 (drastically easier to design) [ 192 , 193 ], it is now possible to control epigenetic modifications at a single gene in a specific type of cell in a specific brain region [ 162 ]. Heller et al. demonstrated that gene-targeted epigenetic editing (targeted to the Fosb [ 194 ] and Cdk5 [ 195 ] locus with ZFP technology) can alter drug-related behaviours [ 194 , 195 ]. This represents crucial evidence that gene-specific changes to the epigenome are not simply correlated, but rather causal, in regulating transcriptional responses to drugs of abuse administrations. These new results of “causal epigenomics” are very encouraging as they open the way to precise translational therapeutic approaches for drug addiction and other CNS diseases.
Linking epigenetics and synaptic plasticity
Today, most studies investigate synaptic plasticity and epigenetic as two distinct fields and it is not clear how these research topics are connected to each other. Understanding how epigenetics is connected to synaptic plasticity is an emerging research issue [ 6 ].
Of course, bridging epigenetic mechanisms with synaptic plasticity is not limited to drug addiction field. For example, in 2011, Monsey et al. [ 196 ] elegantly demonstrated that DNA methylation and histone H3 acetylation regulate auditory fear conditioning and its related synaptic plasticity in the amygdala. In 2014, Massart et al. [ 197 ] suggested that sleep deprivation induces epigenetic modification (alteration in DNA methylation and hydroxymethylation) that triggers synaptic plasticity modifications by changing expression of plasticity related genes.
Regarding drug addiction, some epigenetic marks seem fundamental and upstream as illustrated by HDAC inhibitors effect on drug-induced synaptic and behavioural modifications [ 178 , 198 , 199 , 200 ]. Additionally, Maze et al. [ 201 ] demonstrated morphological plasticity induced by cocaine through the histone methyltransferase G9a. Again advocating for causal epigenetic, Authement et al. [ 66 ] demonstrated that HDAC inhibition locally in the VTA is sufficient to reverse epigenetic modifications and synaptic plasticity changes after morphine administration.
Two transcription factors implicated in addiction exemplify this bridging attempt: CREB and ∆FosB (a truncated form of the FosB gene) are both activated by several drugs of abuse [ 202 ]. CREB activation occurs in both subtypes of NAc MSNs (D1R and D2R), while ∆FosB activation is limited to D1R MSNs in response to all drugs of abuse except for opioids, which remarkably induce the protein in both MSNs [ 203 ]. Expression of active CREB in NAc MSNs increases their excitability [ 204 ] and underlies drug-induced long-term synaptic plasticity and associated changes in dendritic spine plasticity [ 205 ]. ∆FosB is also linked to synaptic plasticity but evokes contrasting effects on the two MSN subtypes, with increased AMPA receptor function induced in D1R MSNs and decreased AMPA receptor function induced in D2R MSNs [ 206 ]. Renthal et al. [ 150 ] unravelled CREB and ∆FosB target genes and observed that these genes are mainly involved in neuronal excitability and synaptic function. Moreover, as already briefly discussed above, CREB and ∆FosB action have also been related to multiple epigenetic regulations, including histone acetylation and methylation [ 150 ]. Besides, a novel mechanism for bridging the gap between epigenetic control of transcription and synapse plasticity might be seen in microRNAs [ 207 ]. The most studied miRNA in the context of synaptic plasticity is miR-132 and is known to be CREB-dependent [ 208 ]. In the striatum, miR-212 targets the epigenetic regulator methyl CpG binding protein 2 (MeCP2). MeCP2 acts as a transcriptional repressor through recruitment of histone deacetylases to methylated DNA segments [ 209 , 210 ].
Clinical treatments for drug addiction
Besides psychosocial interventions [ 211 ] such as cognitive behavioural therapy, the most widely used treatment for drug addiction involves agonist-like medication, a solution inadequately called replacement or substitution therapy [ 212 ]. This type of treatment has been successfully implemented in the daily practice for opioid use disorder (e.g.: methadone, buprenorphine) [ 213 ] and tobacco use disorder (e.g.: nicotine patch or gum, varenicline) [ 214 ]. Currently, this agonist-like treatment is also promising for psychostimulant use disorder [ 215 ]. Still, considering the addictive drug-like effect, the risk of abuse, misuse and diversion, replacement therapy should be prescribed with caution [ 215 , 216 ].
Recently, a randomised and control study on a cocaine vaccine failed to show an effectiveness but instead raised an important issue: immunised subjects may have increased their cocaine use to overcome the competitive anti-cocaine antibody inhibition [ 217 ]. Even though significant improvements have been developed for immunopharmacotherapies for psychostimulant addiction over the last decade, very few candidates have been evaluated so far in clinical trials [ 218 ]. These considerations are some of the reasons why other treatments for drug addiction should emerge with the help of neurobiological research [ 219 ].
Following successful subthalamic nucleus DBS for Parkinson’s disease [ 220 , 221 , 222 ], DBS was investigated for diverse psychiatric diseases including depression [ 223 ], obsessive-compulsive disorder [ 224 ] and Tourette syndrome [ 225 ]. Today, indications for DBS are enlarging, with several positive case reports and small cases series that studied NAc DBS for drug addiction. The first studies showing potential positive effects on drug addiction were reports on application of NAc DBS primarily intended for other medication-refractory neuropsychiatric disorder where a comorbid drug addiction was unexpectedly resolved [ 226 , 227 ]. For DBS treatment in drug addiction, it seems that clinical empirical results led to further bench investigations and refinement [ 88 , 103 , 228 , 229 , 230 , 231 ], or at least, clinical and animal studies evolved in parallel with poor connectivity between the two.
Afterwards, many case reports and small cases series studied NAc DBS being used primarily for drug addiction, all showing encouraging decreases in drug use [ 232 , 233 , 234 , 235 , 236 , 237 ]. However, these studies are limited by their descriptive nature, inconstant follow-up, multiple publication bias, small patient numbers and lack of blinded stimulation and standardised outcome measures. At this stage, additional preclinical and clinical research are needed to clarify the role of DBS in the treatment of drug addiction [ 237 ]. Currently, randomised and control clinical studies are conducted (NCT01245075).
In a recent review, Sanna et al. [ 238 ] highlighted how repetitive transcranial magnetic stimulation (rTMS) confirms the hypodopaminergic hypothesis of drug addiction. While enhancing dopaminergic function through direct or indirect pharmacological approaches does not significantly alleviate symptoms, in numerous studies, and has not yielded a single FDA-approved medication [ 239 ], rTMS might indirectly modulate the dopaminergic system. Many rTMS studies stimulate the dorsolateral PFC [ 240 , 241 ] that projects to the VTA and thus induces an increase in dopamine release in the synaptic cleft in the NAc [ 55 , 242 , 243 ]. Nevertheless, considering the heterogeneity of methods used in rTMS studies during the last 10 years [ 238 ], protocols and guidelines, were recently suggested by an international network of experts in neuromodulation and addiction to improve homogeneity of studies [ 244 ]. From this report, it is clear that multiple technical details for optimal stimulation need further investigations that might be achieved through preclinical studies. For example, low frequency (but not high-frequency) rTMS before methamphetamine exposure in rats blocked drug-induced conditioned place preference [ 245 ]. Being non-invasive, with insignificant side effects, rTMS could be seen as a great opportunity for drug addiction treatment. We are currently waiting for the results of a randomised and control study that aims at determine if, in heavy alcohol users, a single session of TMS can lower a patient’s craving and brain response to alcohol cues (NCT02939313).
Interesting views of clinical treatments for drug addiction are discussed in some other reviews [ 212 , 215 , 216 , 219 ]. The clinical impact of new treatments also depends on their translation into clinical practice which is mainly promoted by the pharmaceutical industry [ 219 ]. Indeed, even when an effective treatment is identified through basic research, it is commonly challenging to translate it to clinical practice, as illustrated by naltrexone as a treatment of alcoholism [ 219 ]. Another example of problematic translation to clinic is illustrated by modafinil, a treatment that has been reported to attenuate cocaine euphoria but for which larger clinical randomised and controlled studies showed controversial results [ 246 , 247 ].
Future directions
Drug addiction is a brain disease strongly influenced by environment and psychosocial aspects. The psychosocial conditions in which it has developed are extremely important. Exposure to conditioned cues can be a central issue in causing drug cravings and relapses, even after successful treatment, and thus they have to be minimised [ 2 , 74 , 77 ]. The pathophysiological aspects are particularly unsteady. For instance, as discussed in this review and in other ones [ 73 , 248 ], synaptic plasticity is dynamically altered after psychostimulant administration, so that a treatment could have opposite effects depending on timing aspects of the administration protocol. In addition, a prolonged treatment may involve compensatory mechanisms, giving unexpected results (e.g.: when HDAC inhibitors and psychostimulants are both administered acutely, they have synergistic effects through hyperacetylation and thus transcriptional activation of psychostimulant-regulated target genes. Conversely, when a drug of abuse is given in the context of chronic HDAC inhibitor, compensatory mechanisms may promote acetylated histone to the promoters of genes responsible for inducing histone methylation and thus chromatin condensation and gene repression, all of which, in turn, gave opposite effect [ 183 ]). Thus, the evolution through the different stages of the disease has to be taken into account [ 249 ] and treatment must follow them. These two aspects have to be incorporated in a holistic treatment strategy. Besides, studying combination of different cutting-edge approaches, with animal models of addiction, such as targeted rTMS or DBS with more systemic epigenetic modulation might show a better restoration of altered synaptic transmission and decrease the probability of relapse in drug addiction. Basically, drug addiction is a disease that seems to be difficult to treat preventively but it is more conceivable to help patients that would be in an abstinence stage not to experience relapse of their disease. As addiction is chronic and relapsing, a good treatment outcome is a significant reduction of drug administration and long periods of withdrawal, with only sporadic relapses [ 2 ].
It is clear that the main issues for optimal therapeutic management of this specific psychiatric disease belong to its dynamic complexity, diverse temporal evolution and undeniably psychosocial aspects. In this review, we focused mostly on the effects of drugs of abuse on synaptic plasticity and epigenetic modifications. Nowadays, these two subfields are mostly studied separately and the understanding of how these two main addictive drug-induced brain modifications interact might be fundamental for addiction research [ 6 ]. Indeed, argument for clinical trials for new treatments emerge from fundamental behavioural studies that should be implemented in a global approach to the addicted patient.
Conclusions
Here, we highlight, from a vast fundamental literature (mainly based on rodent models), promising therapeutics that would potentially treat drug addiction. Based on effect, on synaptic plasticity and epigenetic mechanisms, treatments such as GluA2-lacking AMPAR antagonists [ 72 , 84 ], mGluR1 positive allosteric modulator [ 85 ], NAc 12Hz-DBS [ 103 ] (in line with other promising neuromodulation therapeutics such as rTMS or transcranial direct current stimulation [ 250 ]), N-acetylcysteine [ 108 ], HDAC inhibitors [ 183 ] or even (in very early stages of investigation) CRISPR/dCas9 epigenetic editing [ 194 , 195 ] could be potential candidates for human randomised clinical trials (Fig. 3 ).
Finally, it is fundamental to consider the specific clinical aspects of the disease that would help to develop a personalised-treatment strategy. Indeed, after going from the bench to the bedside it will also be essential to assess the reversed route.
Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–88.
Article Google Scholar
Leshner AI. Addiction is a brain disease, and it matters. Science. 1997;278:45–47.
Article CAS PubMed Google Scholar
Nielsen DA, Nielsen EM, Dasari T, Spellicy CJ. Pharmacogenetics of addiction therapy. Methods Mol Biol. 2014;1175:589–624.
Article PubMed CAS Google Scholar
Everitt BJ & Robbins TW. Drug addiction: updating actions to habits to compulsions ten years on. Annu Rev Psychol. 2015;67:23–50.
Article PubMed Google Scholar
Belin D, Everitt BJ. Cocaine seeking habits depend upon dopamine-dependent serial connectivity linking the ventral with the dorsal striatum. Neuron. 2008;57:432–41.
Nestler EJ, Lüscher C. The molecular basis of drug addiction: linking epigenetic to synaptic and circuit mechanisms. Neuron. 2019;102:48–59.
Article CAS PubMed PubMed Central Google Scholar
Nestler EJ. Cellular basis of memory for addiction. Dialogues Clin Neurosci. 2013;15:431–43.
Article PubMed PubMed Central Google Scholar
Nestler EJ. Molecular basis of long-term plasticity underlying addiction. Nat Rev Neurosci. 2001;2:119–28.
Anthony JC, Warner LA, Kessler RC. Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: basic findings from the National Comorbidity Survey. Exp Clin Psychopharmacol. 1994;2:244–68.
Egervari G, Ciccocioppo R, Jentsch JD, Hurd YL. Shaping vulnerability to addiction – the contribution of behavior, neural circuits and molecular mechanisms. Neurosci Biobehav Rev. 2018;85:117–25.
Li MD, Burmeister M. New insights into the genetics of addiction. Nat. Rev. Genet. 2009;10:225–31.
Kreek MJ, Nielsen DA, Butelman ER, LaForge KS. Genetic influences on impulsivity, risk taking, stress responsivity and vulnerability to drug abuse and addiction. Nat Neurosci. 2005;8:1450–7.
Shohat S, Amelan A, Shifman S. Convergence and divergence in the genetics of psychiatric disorders from pathways to developmental stages. Biol Psychiatry. 2021;89:32–40.
Kandel, DB. Stages and Pathways of Drug Involvement: Examining the Gateway Hypothesis (Cambridge University Press, 2002).
Gerfen CR, Engber TM, Mahan LC, Susel Z, Chase TN, Monsma FJ Jr, et al. D1 and D2 dopamine receptor-regulated gene expression of striatonigral and striatopallidal neurons. Science. 1990;250:1429–32.
Schiffmann SN, Fisone G, Moresco R, Cunha RA, Ferré S. Adenosine A2A receptors and basal ganglia physiology. Prog. Neurobiol. 2007;83:277–92.
Gerfen CR, Surmeier DJ. Modulation of striatal projection systems by dopamine. Annu Rev Neurosci. 2011;34:441–66.
Di Chiara G, Imperato A. Drugs abused by humans preferentially increase synaptic dopamine concentrations in the mesolimbic system of freely moving rats. Proc Natl Acad Sci USA. 1988;85:5274–8.
Tanda G, Pontieri FE, Chiara GD. Cannabinoid and heroin activation of mesolimbic dopamine transmission by a common µ1 opioid receptor mechanism. Science. 1997;276:2048–50.
Pontieri FE, Tanda G, Orzi F, Chiara GD. Effects of nicotine on the nucleus accumbens and similarity to those of addictive drugs. Nature. 1996;382:255–7.
Nestler EJ. Is there a common molecular pathway for addiction? Nat Neurosci. 2005;8:1445–9.
Nestler EJ. The neurobiology of cocaine addiction. Sci Pract Perspect. 2005;3:4–10.
Kalivas PW, Volkow N, Seamans J. Unmanageable motivation in addiction: a pathology in prefrontal-accumbens glutamate transmission. Neuron. 2005;45:647–50.
Volkow ND, Fowler JS, Wang G-J, Swanson JM. Dopamine in drug abuse and addiction: results from imaging studies and treatment implications. Mol Psychiatry. 2004;9:557–69.
Chen SA, O'Dell LE, Hoefer ME, Greenwell TN, Zorrilla EP, Koob GF. Unlimited access to heroin self-administration: independent motivational markers of opiate dependence. Neuropsychopharmacology. 2006;31:2692–707.
Laviolette SR, Alexson TO, van der Kooy D. Lesions of the tegmental pedunculopontine nucleus block the rewarding effects and reveal the aversive effects of nicotine in the ventral tegmental area. J. Neurosci. 2002;22:8653–60.
Koob GF, Volkow ND. Neurocircuitry of addiction. Neuropsychopharmacology. 2010;35:217–38.
Pierce RC, Kumaresan V. The mesolimbic dopamine system: The final common pathway for the reinforcing effect of drugs of abuse? Neurosci Biobehav Rev. 2006;30:215–38.
Belin-Rauscent A, Fouyssac M, Bonci A, Belin D. How preclinical models evolved to resemble the diagnostic criteria of drug addiction. Biol. Psychiatry. 2016;79:39–46.
Piazza PV, Deroche-Gamonet V. A multistep general theory of transition to addiction. Psychopharmacology. 2013;229:387–413.
Pascoli V, Hiver A, Van Zessen R, Loureiro M, Achargui R, Harada M, et al. Stochastic synaptic plasticity underlying compulsion in a model of addiction. Nature. 2018;564:366–71.
Kauer JA, Malenka RC. Synaptic plasticity and addiction. Nat Rev Neurosci. 2007;8:844–58.
Mameli M, Balland B, Luján R, Lüscher C. Rapid synthesis and synaptic insertion of GluR2 for mGluR-LTD in the ventral tegmental area. Science. 2007;317:530–3.
Bellone C, Lüscher C. Cocaine triggered AMPA receptor redistribution is reversed in vivo by mGluR-dependent long-term depression. Nat Neurosci. 2006;9:636–41.
Pignatelli M, Bonci A. Role of dopamine neurons in reward and aversion: a synaptic plasticity perspective. Neuron. 2015;86:1145–57.
Stuber GD, Klanker M, de Ridder B, Bowers MS, Joosten RN, Feenstra MG, et al. Reward-predictive cues enhance excitatory synaptic strength onto midbrain dopamine neurons. Science. 2008;321:1690–2.
Bolam JP, Smith Y. The GABA and substance P input to dopaminergic neurones in the substantia nigra of the rat. Brain Res. 1990;529:57–78.
Henny P, Brown MT, Northrop A, Faunes M, Ungless MA, Magill PJ, et al. Structural correlates of heterogeneous in vivo activity of midbrain dopaminergic neurons. Nat Neurosci. 2012;15:613–9.
Bayer VE, Pickel VM. GABA-labeled terminals form proportionally more synapses with dopaminergic neurons containing low densities of tyrosine hydroxylase-immunoreactivity in rat ventral tegmental area. Brain Res. 1991;559:44–55.
Johnson SW, North RA. Two types of neurone in the rat ventral tegmental area and their synaptic inputs. J Physiol. 1992;450:455–68.
Edwards NJ, Tejeda HA, Pignatelli M, Zhang S, McDevitt RA, Wu J, et al. Circuit specificity in the inhibitory architecture of the VTA regulates cocaine-induced behavior. Nat Neurosci. 2017;20:438–48.
Menegas W, Bergan JF, Ogawa SK, Isogai Y, Umadevi Venkataraju K, Osten P, et al. Dopamine neurons projecting to the posterior striatum form an anatomically distinct subclass. eLife. 2015;4:e10032.
Ling W, Shoptaw S, Majewska D. Baclofen as a cocaine anti-craving medication: a preliminary clinical study. Neuropsychopharmacology. 1998;18:403–4.
CAS PubMed Google Scholar
Young KA, Franklin TR, Roberts DC, Jagannathan K, Suh JJ, Wetherill RR, et al. Nipping cue reactivity in the bud: baclofen prevents limbic activation elicited by subliminal drug cues. J Neurosci. 2014;34:5038–43.
Article PubMed PubMed Central CAS Google Scholar
Vocci FJ, Elkashef A. Pharmacotherapy and other treatments for cocaine abuse and dependence. Curr Opin Psychiatry. 2005;18:265–70.
Roberts DC, Andrews MM, Vickers GJ. Baclofen attenuates the reinforcing effects of cocaine in rats. Neuropsychopharmacology. 1996;15:417–23.
Slattery DA, Markou A, Froestl W, Cryan JF. The GABA B receptor-positive modulator GS39783 and the GABA B receptor agonist baclofen attenuate the reward-facilitating effects of cocaine: intracranial self-stimulation studies in the rat. Neuropsychopharmacology. 2005;30:2065–72.
Hotsenpiller G, Wolf ME. Baclofen attenuates conditioned locomotion to cues associated with cocaine administration and stabilizes extracellular glutamate levels in rat nucleus accumbens. Neuroscience. 2003;118:123–34.
Brebner K, Phelan R, Roberts DCS. Intra-VTA baclofen attenuates cocaine self-administration on a progressive ratio schedule of reinforcement. Pharmacol Biochem Behav. 2000;66:857–62.
Penn RD, Savoy SM, Corcos D, Latash M, Gottlieb G, Parke B, et al. Intrathecal baclofen for severe spinal spasticity. N Engl J Med. 1989;320:1517–21.
Sammaraiee Y, Yardley M, Keenan L, Buchanan K, Stevenson V, Farrell R. Intrathecal baclofen for multiple sclerosis related spasticity: a twenty year experience. Mult Scler Relat Disord. 2019;27:95–100.
Reynoard J, Schmitt C, Torrents R, Simon N. Toxicological considerations in the prescription of baclofen for the treatment of substance use disorders. Expert Opin Drug Metab Toxicol. 2020;16:309–17.
Garbutt JC, Kampov-Polevoy AB, Gallop R, Kalka-Juhl L, Flannery BA. Efficacy and safety of baclofen for alcohol dependence: a randomized, double-blind, placebo-controlled trial. Alcohol Clin Exp Res. 2010;34:1849–57.
Yamini D, Lee SH, Avanesyan A, Walter M, Runyon B. Utilization of baclofen in maintenance of alcohol abstinence in patients with alcohol dependence and alcoholic hepatitis with or without cirrhosis. Alcohol Alcohol. 2014;49:453–6.
Addolorato G, Leggio L, Hopf FW, Diana M, Bonci A. Novel therapeutic strategies for alcohol and drug addiction: focus on GABA, ion channels and transcranial magnetic stimulation. Neuropsychopharmacology. 2012;37:163–77.
Kahn R, Biswas K, Childress AR, Shoptaw S, Fudala PJ, Gorgon L, et al. Multi-center trial of baclofen for abstinence initiation in severe cocaine-dependent individuals. Drug Alcohol Depend. 2009;103:59–64.
Dore GM, Lo K, Juckes L, Bezyan S, Latt N. Clinical experience with baclofen in the management of alcohol-dependent patients with psychiatric comorbidity: a selected case series. Alcohol Alcohol. 2011;46:714–20.
Nugent FS, Penick EC, Kauer JA. Opioids block long-term potentiation of inhibitory synapses. Nature. 2007;446:1086–90.
Liu Q, Pu L, Poo M. Repeated cocaine exposure in vivo facilitates LTP induction in midbrain dopamine neurons. Nature. 2005;437:1027–31.
Barrett AC, Negus SS, Mello NK, Caine SB. Effect of GABA agonists and GABA-A receptor modulators on cocaine- and food-maintained responding and cocaine discrimination in rats. J Pharmacol Exp Ther. 2005;315:858–71.
Brodie JD, Figueroa E, Dewey SL. Treating cocaine addiction: from preclinical to clinical trial experience with γ-vinyl GABA. Synapse. 2003;50:261–5.
Barker JS, Hines RM. Regulation of GABAA receptor subunit expression in substance use disorders. Int J Mol Sci. 2020;21:4445.
Article CAS PubMed Central Google Scholar
Tan KR, Rudolph U, Lüscher C. Hooked on benzodiazepines: GABAA receptor subtypes and addiction. Trends Neurosci. 2011;34:188–97.
Brands B, Blake J, Marsh DC, Sproule B, Jeyapalan R, Li S. The impact of benzodiazepine use on methadone maintenance treatment outcomes. J Addict Dis. 2008;27:37–48.
Dacher M, Nugent FS. Morphine-induced modulation of LTD at GABAergic synapses in the ventral tegmental area. Neuropharmacology. 2011;61:1166–71.
Authement ME, Langlois LD, Kassis H, Gouty S, Dacher M, Shepard RD, et al. Morphine-induced synaptic plasticity in the VTA is reversed by HDAC inhibition. J Neurophysiol. 2016;116:1093–103.
Abraham WC, Bear MF. Metaplasticity: the plasticity of synaptic plasticity. Trends Neurosci. 1996;19:126–30.
Martin M, Chen BT, Hopf FW, Bowers MS, Bonci A. Cocaine self-administration selectively abolishes LTD in the core of the nucleus accumbens. Nat. Neurosci. 2006;9:868–9.
Thomas MJ, Beurrier C, Bonci A, Malenka RC. Long-term depression in the nucleus accumbens: a neural correlate of behavioral sensitization to cocaine. Nat. Neurosci. 2001;4:1217–23.
Boudreau AC, Wolf ME. Behavioral sensitization to cocaine is associated with increased AMPA receptor surface expression in the nucleus accumbens. J. Neurosci. 2005;25:9144–51.
Ferrario CR, Li X, Wang X, Reimers JM, Uejima JL, Wolf ME. The role of glutamate receptor redistribution in locomotor sensitization to cocaine. Neuropsychopharmacology. 2010;35:818–33.
Conrad KL, Tseng KY, Uejima JL, Reimers JM, Heng LJ, Shaham Y, et al. Formation of accumbens GluR2-lacking AMPA receptors mediates incubation of cocaine craving. Nature. 2008;454:118–21. https://doi.org/10.1038/nature06995 .
Wolf ME, Tseng KY. Calcium-permeable AMPA receptors in the VTA and nucleus accumbens after cocaine exposure:when, how, and why? Front Mol Neurosci. 2012;5:72.
Grimm JW, Hope BT, Wise RA, Shaham Y. Neuroadaptation. Incubation of cocaine craving after withdrawal. Nature. 2001;412:141–2.
Sadler-Smith E. Wallas’ four-stage model of the creative process: more than meets the eye? Creat Res J. 2015;27:342–52.
Gawin FH, Kleber HD. Abstinence symptomatology and psychiatric diagnosis in cocaine abusers. Clinical observations. Arch Gen Psychiatry. 1986;43:107–13.
Childress AR, Mozley PD, McElgin W, Fitzgerald J, Reivich M, O'Brien CP. Limbic activation during cue-induced cocaine craving. Am J Psychiatry. 1999;156:11–18.
Parvaz MA, Moeller SJ, Goldstein RZ. Incubation of cue-induced craving in adults addicted to cocaine measured by electroencephalography. JAMA Psychiatry. 2016;73:1127–34.
Lippman-Bell JJ, Zhou C, Sun H, Feske JS, Jensen FE. Early-life seizures alter synaptic calcium-permeable AMPA receptor function and plasticity. Mol Cell Neurosci. 2016;76:11–20.
Achuta VS, Möykkynen T, Peteri UK, Turconi G, Rivera C, Keinänen K, et al. Functional changes of AMPA responses in human induced pluripotent stem cell-derived neural progenitors in fragile X syndrome. Sci Sÿignal. 2018;11:eaan8784.
Article CAS Google Scholar
Selvaraj BT, Livesey MR, Zhao C, Gregory JM, James OT, Cleary EM, et al. C9ORF72 repeat expansion causes vulnerability of motor neurons to Ca 2+ -permeable AMPA receptor-mediated excitotoxicity. Nat Commun. 2018;9:347.
Kobylecki C, Cenci MA, Crossman AR, Ravenscroft P. Calcium-permeable AMPA receptors are involved in the induction and expression of l-DOPA-induced dyskinesia in Parkinson’s disease. J Neurochem. 2010;114:499–511.
Whitehead G, Regan P, Whitcomb DJ, Cho K. Ca2+-permeable AMPA receptor: a new perspective on amyloid-beta mediated pathophysiology of Alzheimer’s disease. Neuropharmacology. 2017;112:221–7.
Twomey EC, Yelshanskaya MV, Vassilevski AA, Sobolevsky AI. Mechanisms of channel block in calcium-permeable AMPA receptors. Neuron. 2018;99:956–.e4.
Loweth JA, Scheyer AF, Milovanovic M, LaCrosse AL, Flores-Barrera E, Werner CT, et al. Synaptic depression via mGluR1 positive allosteric modulation suppresses cue-induced cocaine craving. Nat. Neurosci. 2014;17:73–80.
Scheyer AF, Loweth JA, Christian DT, Uejima J, Rabei R, Le T, et al. AMPA receptor plasticity in accumbens core contributes to incubation of methamphetamine craving. Biol. Psychiatry. 2016;80:661–70.
Pascoli V, Terrier J, Espallergues J, Valjent E, O'Connor EC, Lüscher C. Contrasting forms of cocaine-evoked plasticity control components of relapse. Nature. 2014;509:459–64.
Ma T, Cheng Y, Roltsch Hellard E, Wang X, Lu J, Gao X, et al. Bidirectional and long-lasting control of alcohol-seeking behavior by corticostriatal LTP and LTD. Nat. Neurosci. 2018;21:373–83.
Pascoli V, Turiault M, Lüscher C. Reversal of cocaine-evoked synaptic potentiation resets drug-induced adaptive behaviour. Nature. 2012;481:71–75.
Valjent E, Bertran-Gonzalez J, Aubier B, Greengard P, Hervé D, Girault JA. Mechanisms of locomotor sensitization to drugs of abuse in a two-injection protocol. Neuropsychopharmacology 2010;35:401–15.
Robinson TE, Berridge KC. The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Res Brain Res Rev. 1993;18:247–91.
Schenk S, Partridge B. Sensitization and tolerance in psychostimulant self-administration. Pharmacol Biochem Behav. 1997;57:543–50.
Vezina P, Lorrain DS, Arnold GM, Austin JD, Suto N. Sensitization of midbrain dopamine neuron reactivity promotes the pursuit of amphetamine. J Neurosci. 2002;22:4654–62.
De Vries TJ, Schoffelmeer AN, Binnekade R, Mulder AH, Vanderschuren LJ. Drug-induced reinstatement of heroin- and cocaine-seeking behaviour following long-term extinction is associated with expression of behavioural sensitization. Eur J Neurosci. 1998;10:3565–71.
Suto N, Tanabe LM, Austin JD, Creekmore E, Pham CT, Vezina P. Previous exposure to psychostimulants enhances the reinstatement of cocaine seeking by nucleus accumbens AMPA. Neuropsychopharmacology. 2004;29:2149–59.
Vorspan F, de Witt P, Zerdazi EH, Karsinti E, Ksouda K, Icick R, et al. Chronic exposure to cocaine is associated with persistent behavioral disturbances. A cross-sectional dimensional study in outpatients with multiple substance use disorders. Psychopharmacology. 2020;237:3399–407.
Vorspan F, Icick R, Mekdad N, Courtin C, Bloch V, Bellivier F, et al. Translational study of the whole transcriptome in rats and genetic polymorphisms in humans identifies LRP1B and VPS13A as key genes involved in tolerance to cocaine-induced motor disturbances. Transl Psychiatry. 2020;10:381.
Vanderschuren LJ, Kalivas PW. Alterations in dopaminergic and glutamatergic transmission in the induction and expression of behavioral sensitization: a critical review of preclinical studies. Psychopharmacology. 2000;151:99–120.
Vezina P, Leyton M. Conditioned cues and the expression of stimulant sensitization in animals and humans. Neuropharmacology. 2009;56:160–8.
Tzschentke TM. REVIEW ON CPP: measuring reward with the conditioned place preference (CPP) paradigm: update of the last decade. Addict Biol. 2007;12:227–462.
Bardo MT, Bevins RA. Conditioned place preference: what does it add to our preclinical understanding of drug reward? Psychopharmacology. 2000;153:31–43.
Itzhak Y, Martin JL. Cocaine-induced conditioned place preference in mice: induction, extinction and reinstatement by related psychostimulants. Neuropsychopharmacology. 2002;26:130–4.
Creed M, Pascoli VJ, Lüscher C. Refining deep brain stimulation to emulate optogenetic treatment of synaptic pathology. Science. 2015;347:659–64.
Shen Y, Campbell RE, Côté DC, Paquet M-E. Challenges for therapeutic applications of opsin-based optogenetic tools in humans. Front Neural Circuits. 2020;14:41.
Vorspan F, Mallet L, Corvol J-C, Pelissolo A, Lépine J-P. Treating addictions with deep brain stimulation is premature but well-controlled clinical trials should be performed. Addict Abingdon Engl. 2011;106:1535–6.
Mahoney JJ, Hanlon CA, Marshalek PJ, Rezai AR, Krinke L. Transcranial magnetic stimulation, deep brain stimulation, and other forms of neuromodulation for substance use disorders: review of modalities and implications for treatment. J Neurol Sci. 2020;418:117149.
Shen W, Flajolet M, Greengard P, Surmeier DJ. Dichotomous dopaminergic control of striatal synaptic plasticity. Science. 2008;321:848–51.
Moussawi K, Pacchioni A, Moran M, Olive MF, Gass JT, Lavin A, et al. N -Acetylcysteine reverses cocaine-induced metaplasticity. Nat Neurosci. 2009;12:182–9.
Gerfen CR. The neostriatal mosaic: multiple levels of compartmental organization. Trends Neurosci. 1992;15:133–9.
Vicente AM, Galvão-Ferreira P, Tecuapetla F, Costa RM. Direct and indirect dorsolateral striatum pathways reinforce different action strategies. Curr Biol. 2016;26:R267–269.
Freeze BS, Kravitz AV, Hammack N, Berke JD, Kreitzer AC. Control of basal ganglia output by direct and indirect pathway projection neurons. J Neurosci. 2013;33:18531–9.
Durieux PF, Schiffmann SN, de Kerchove d’Exaerde A. Differential regulation of motor control and response to dopaminergic drugs by D1R and D2R neurons in distinct dorsal striatum subregions. EMBO J. 2012;31:640–53.
Cox J, Witten IB. Striatal circuits for reward learning and decision-making. Nat Rev Neurosci. 2019;20:482–94.
Lalchandani RR, van der Goes M-S, Partridge JG, Vicini S. Dopamine D2 receptors regulate collateral inhibition between striatal medium spiny neurons. J Neurosci. 2013;33:14075–86.
Dobbs LK, Kaplan AR, Lemos JC, Matsui A, Rubinstein M, Alvarez VA. Dopamine regulation of lateral inhibition between striatal neurons gates the stimulant actions of cocaine. Neuron. 2016;90:1100–13.
Dobbs LK, Kaplan AR, Bock R, Phamluong K, Shin JH, Bocarsly ME, et al. D1 receptor hypersensitivity in mice with low striatal D2 receptors facilitates select cocaine behaviors. Neuropsychopharmacology. 2019;44:805–16.
Tecuapetla F, Koós T, Tepper JM, Kabbani N, Yeckel MF. Differential dopaminergic modulation of neostriatal synaptic connections of striatopallidal axon collaterals. J Neurosci. 2009;29:8977–90.
Mulholland PJ, Chandler LJ, Kalivas PW. Signals from the fourth dimension regulate drug relapse. Trends Neurosci. 2016;39:472–85.
Smith AC, Kupchik YM, Scofield MD, Gipson CD, Wiggins A, Thomas CA, et al. Synaptic plasticity mediating cocaine relapse requires matrix metalloproteinases. Nat Neurosci. 2014;17:1655–7.
Moussawi K, Zhou W, Shen H, Reichel CM, See RE, Carr DB, et al. Reversing cocaine-induced synaptic potentiation provides enduring protection from relapse. Proc Natl Acad Sci USA. 2011;108:385–90.
Abulseoud OA, Camsari UM, Ruby CL, Kasasbeh A, Choi S, Choi DS. Attenuation of ethanol withdrawal by ceftriaxone-induced upregulation of glutamate transporter EAAT2. Neuropsychopharmacology. 2014;39:1674–84.
Knackstedt LA, Melendez RI, Kalivas PW. Ceftriaxone restores glutamate homeostasis and prevents relapse to cocaine seeking. Biol Psychiatry. 2010;67:81–84.
Huntley GW. Synaptic circuit remodelling by matrix metalloproteinases in health and disease. Nat. Rev. Neurosci. 2012;13:743–57.
Brown TE, Forquer MR, Harding JW, Wright JW, Sorg BA. Increase in matrix metalloproteinase-9 levels in the rat medial prefrontal cortex after cocaine reinstatement of conditioned place preference. Synapse. 2008;62:886–9.
Mizoguchi H, Yamada K, Mouri A, Niwa M, Mizuno T, Noda Y, et al. Role of matrix metalloproteinase and tissue inhibitor of MMP in methamphetamine-induced behavioral sensitization and reward: implications for dopamine receptor down-regulation and dopamine release. J Neurochem. 2007;102:1548–60.
Kroener S, Mulholland PJ, New NN, Gass JT, Becker HC, Chandler LJ. Chronic alcohol exposure alters behavioral and synaptic plasticity of the rodent prefrontal cortex. PLoS ONE. 2012;7:e37541.
Nimitvilai S, Lopez MF, Mulholland PJ, Woodward JJ. Chronic intermittent ethanol exposure enhances the excitability and synaptic plasticity of lateral orbitofrontal cortex neurons and induces a tolerance to the acute inhibitory actions of ethanol. Neuropsychopharmacology. 2016;41:1112–27.
Kasanetz F, Lafourcade M, Deroche-Gamonet V, Revest JM, Berson N, Balado E, et al. Prefrontal synaptic markers of cocaine addiction-like behavior in rats. Mol Psychiatry. 2013;18:729–37.
Meinhardt MW, Hansson AC, Perreau-Lenz S, Bauder-Wenz C, Stählin O, Heilig M, et al. Rescue of infralimbic mGluR2 deficit restores control over drug-seeking behavior in alcohol dependence. J Neurosci. 2013;33:2794–806.
Lu L, Uejima JL, Gray SM, Bossert JM, Shaham Y. Systemic and central amygdala injections of the mGluR2/3 agonist LY379268 attenuate the expression of incubation of cocaine craving. Biol Psychiatry. 2007;61:591–8.
Baptista MAS, Martin-Fardon R, Weiss F. Preferential effects of the metabotropic glutamate 2/3 receptor agonist LY379268 on conditioned reinstatement versus primary reinforcement: comparison between cocaine and a potent conventional reinforcer. J Neurosci. 2004;24:4723–7.
Peters J, Kalivas PW. The group II metabotropic glutamate receptor agonist, LY379268, inhibits both cocaine- and food-seeking behavior in rats. Psychopharmacology. 2006;186:143–9.
Caprioli D, Justinova Z, Venniro M, Shaham Y. Effect of novel allosteric modulators of metabotropic glutamate receptors on drug self-administration and relapse: a review of preclinical studies and their clinical implications. Biol Psychiatry. 2018;84:180–92.
Clark AM et al. Dopamine D2 receptors in the paraventricular thalamus attenuate cocaine locomotor sensitization. eNeuro. 2017;4:ENEURO.0227-17.2017.
Dong X, Li S, Kirouac GJ. Collateralization of projections from the paraventricular nucleus of the thalamus to the nucleus accumbens, bed nucleus of the stria terminalis, and central nucleus of the amygdala. Brain Struct. Funct. 2017;222:3927–43.
Huang AS, Mitchell JA, Haber SN, Alia-Klein N & Goldstein RZ. The thalamus in drug addiction: from rodents to humans. Philos Trans R Soc Lond B Biol Sci. 2018;373:20170028.
Perez SM, Lodge DJ. Convergent inputs from the hippocampus and thalamus to the nucleus accumbens regulate dopamine neuron activity. J Neurosci. 2018;38:10607–18.
Kelley AE, Baldo BA, Pratt WE. A proposed hypothalamic–thalamic–striatal axis for the integration of energy balance, arousal, and food reward. J Comp Neurol. 2005;493:72–85.
Penzo MA & Gao C. The paraventricular nucleus of the thalamus: an integrative node underlying homeostatic behavior. Trends Neurosci. 2021. https://doi.org/10.1016/j.tins.2021.03.001 .
De Groote A & de Kerchove d'Exaerde A. Thalamo-Nucleus Accumbens projections in motivated behaviors and addiction. Front Syst Neurosci. 2021;15:711350.
Zhu Y, Wienecke CFR, Nachtrab G, Chen X. A thalamic input to the nucleus accumbens mediates opiate dependence. Nature. 2016;530:219–22.
Chisholm A, Rizzo D, Fortin É, Moman V, Quteishat N, Romano A, et al. Assessing the role of corticothalamic and thalamo-accumbens projections in the augmentation of heroin seeking in chronically food-restricted rats. J Neurosci. 2021;41:354–65.
Otis JM, Zhu M, Namboodiri V, Cook CA, Kosyk O, Matan AM, et al. Paraventricular thalamus projection neurons integrate cortical and hypothalamic signals for cue-reward processing. Neuron. 2019;103:423–.e4.
Giros B, Jaber M, Jones SR, Wightman RM, Caron MG. Hyperlocomotion and indifference to cocaine and amphetamine in mice lacking the dopamine transporter. Nature. 1996;379:606–12.
Sora I, Hall FS, Andrews AM, Itokawa M, Li XF, Wei HB, et al. Molecular mechanisms of cocaine reward: combined dopamine and serotonin transporter knockouts eliminate cocaine place preference. Proc Natl Acad Sci USA. 2001;98:5300–5.
Yang H-J, Zhang HY, Bi GH, He Y, Gao JT, Xi ZX. Deletion of type 2 metabotropic glutamate receptor decreases sensitivity to cocaine reward in rats. Cell Rep. 2017;20:319–32.
Chiamulera C, Epping-Jordan MP, Zocchi A, Marcon C, Cottiny C, Tacconi S, et al. Reinforcing and locomotor stimulant effects of cocaine are absent in mGluR5 null mutant mice. Nat Neurosci. 2001;4:873–4.
De Backer J-F, et al. Deletion of Maged1 in mice abolishes locomotor and reinforcing effects of cocaine. EMBO Rep. 2018;19:e45089.
Karadurmus D, Rial D, De Backer JF, Communi D, de Kerchove d'Exaerde A, Schiffmann SN. GPRIN3 controls neuronal excitability, morphology, and striatal-dependent behaviors in the indirect pathway of the striatum. J. Neurosci. 2019;39:7513–28.
Renthal W, Kumar A, Xiao G, Wilkinson M, Covington HE, Maze I, et al. Genome-wide analysis of chromatin regulation by cocaine reveals a role for sirtuins. Neuron. 2009;62:335–48.
Ena SL, De Backer J-F, Schiffmann SN, de Kerchove d’Exaerde A. FACS array profiling identifies Ecto-5’ nucleotidase as a striatopallidal neuron-specific gene involved in striatal-dependent learning. J Neurosci. 2013;33:8794–809.
Iida, N & Kozasa, T. 29 - Identification and biochemical analysis of GRIN1 and GRIN2. In: Siderovski DP, editor. Methods in Enzymology. Academic Press; 2004;390:475–83.
Mototani Y, Okamura T, Goto M, Shimizu Y, Yanobu-Takanashi R, Ito A, et al. Role of G protein-regulated inducer of neurite outgrowth 3 (GRIN3) in β-arrestin 2-Akt signaling and dopaminergic behaviors. Pflügers Arch. 2018;470:937–47.
Ventura A, Meissner A, Dillon CP, McManus M, Sharp PA, Van Parijs L, et al. Cre-lox-regulated conditional RNA interference from transgenes. Proc Natl Acad Sci USA. 2004;101:10380–5.
David Smith A, Paul Bolam J. The neural network of the basal ganglia as revealed by the study of synaptic connections of identified neurones. Trends Neurosci. 1990;13:259–65.
Robinson TE, Kolb B. Alterations in the morphology of dendrites and dendritic spines in the nucleus accumbens and prefrontal cortex following repeated treatment with amphetamine or cocaine. Eur J Neurosci. 1999;11:1598–604.
Spencer S, Garcia-Keller C, Roberts-Wolfe D, Heinsbroek JA, Mulvaney M, Sorrell A, et al. Cocaine use reverses striatal plasticity produced during cocaine seeking. Biol Psychiatry. 2017;81:616–24.
MacAskill AF, Cassel JM, Carter AG. Cocaine exposure reorganizes cell type– and input-specific connectivity in the nucleus accumbens. Nat Neurosci. 2014;17:1198–207.
Dos Santos M, Cahill EN, Bo GD, Vanhoutte P, Caboche J, Giros B, et al. Cocaine increases dopaminergic connectivity in the nucleus accumbens. Brain Struct Funct. 2018;223:913–23.
Jaenisch R, Bird A. Epigenetic regulation of gene expression: how the genome integrates intrinsic and environmental signals. Nat Genet. 2003;33:245–54.
Nestler EJ. Epigenetic mechanisms of drug addiction. Neuropharmacology. 2014;76:259–68.
Hamilton PJ, Nestler EJ. Epigenetics and addiction. Curr Opin Neurobiol. 2019;59:128–36.
Handel AE, Ramagopalan SV. Is Lamarckian evolution relevant to medicine? BMC Med Genet. 2010;11:73.
Jablonka E & Lamb MJ. Epigenetic Inheritance And Evolution: The Lamarckian Dimension. Oxford University Press; 1999.
Springer JT & Holley D. An Introduction To Zoology: Investigating The Animal World. Jones & Bartlett Learning; 2013.
Vassoler FM, White SL, Schmidt HD, Sadri-Vakili G, Pierce RC. Epigenetic inheritance of a cocaine-resistance phenotype. Nat. Neurosci. 2013;16:42–47.
Goldberg LR, Gould TJ. Multigenerational and transgenerational effects of paternal exposure to drugs of abuse on behavioral and neural function. Eur J Neurosci. 2019;50:2453–66.
Sadri-Vakili G, Kumaresan V, Schmidt HD, Famous KR, Chawla P, Vassoler FM, et al. Cocaine-induced chromatin remodeling increases brain-derived neurotrophic factor transcription in the rat medial prefrontal cortex, which alters the reinforcing efficacy of cocaine. J Neurosci. 2010;30:11735–44.
Schmidt HD, Sangrey GR, Darnell SB, Schassburger RL, Cha JH, Pierce RC, et al. Increased brain-derived neurotrophic factor (BDNF) expression in the ventral tegmental area during cocaine abstinence is associated with increased histone acetylation at BDNF exon I-containing promoters. J Neurochem. 2012;120:202–9.
Gavin DP, et al. Stable histone methylation changes at proteoglycan network genes following ethanol exposure. Front Genet. 2018;9:346.
Sadakierska-Chudy A, Frankowska M, Jastrzębska J, Wydra K, Miszkiel J, Sanak M, et al. Cocaine administration and its withdrawal enhance the expression of genes encoding histone-modifying enzymes and histone acetylation in the rat prefrontal cortex. Neurotox Res. 2017;32:1–10.
Allis CD, Jenuwein T. The molecular hallmarks of epigenetic control. Nat Rev Genet. 2016;17:487–500.
Wang L, Lv Z, Hu Z, Sheng J, Hui B, Sun J, et al. Chronic cocaine-induced H3 acetylation and transcriptional activation of CaMKIIα in the nucleus accumbens is critical for motivation for drug reinforcement. Neuropsychopharmacology. 2010;35:913–28.
Brami-Cherrier K. Parsing molecular and behavioral effects of cocaine in mitogen- and stress-activated protein kinase-1-deficient mice. J Neurosci. 2005;25:11444–54.
Barrett RM, Wood MA. Beyond transcription factors: the role of chromatin modifying enzymes in regulating transcription required for memory. Learn Mem. 2008;15:460–7.
Malvaez M, Mhillaj E, Matheos DP, Palmery M, Wood MA. CBP in the nucleus accumbens regulates cocaine-induced histone acetylation and is critical for cocaine-associated behaviors. J Neurosci. 2011;31:16941–8.
Tsankova NM, Berton O, Renthal W, Kumar A, Neve RL, Nestler EJ. Sustained hippocampal chromatin regulation in a mouse model of depression and antidepressant action. Nat Neurosci. 2006;9:519–25.
Kumar A, Choi KH, Renthal W, Tsankova NM, Theobald DE, Truong HT, et al. Chromatin remodeling is a key mechanism underlying cocaine-induced plasticity in striatum. Neuron. 2005;48:303–14.
Sun J, Wang L, Jiang B, Hui B, Lv Z, Ma L. The effects of sodium butyrate, an inhibitor of histone deacetylase, on the cocaine- and sucrose-maintained self-administration in rats. Neurosci Lett. 2008;441:72–76.
Romieu P, Host L, Gobaille S, Sandner G, Aunis D, Zwiller J. Histone deacetylase inhibitors decrease cocaine but not sucrose self-administration in rats. J. Neurosci. 2008;28:9342–8.
Levine AA, Guan Z, Barco A, Xu S, Kandel ER, Schwartz JH. CREB-binding protein controls response to cocaine by acetylating histones at the fosB promoter in the mouse striatum. Proc Natl Acad Sci USA. 2005;102:19186–91.
Kalda A, Heidmets L-T, Shen H-Y, Zharkovsky A, Chen J-F. Histone deacetylase inhibitors modulates the induction and expression of amphetamine-induced behavioral sensitization partially through an associated learning of the environment in mice. Behav. Brain Res. 2007;181:76–84.
Kennedy PJ, Feng J, Robison AJ, Maze I, Badimon A, Mouzon E, et al. Class I HDAC inhibition blocks cocaine-induced plasticity by targeted changes in histone methylation. Nat Neurosci. 2013;16:434–40.
LaPlant Q, Vialou V, Covington HE, Dumitriu D, Feng J, Warren BL, et al. Dnmt3a regulates emotional behavior and spine plasticity in the nucleus accumbens. Nat Neurosci. 2010;13:1137–43.
Massart R, Barnea R, Dikshtein Y, Suderman M, Meir O, Hallett M, et al. Role of DNA methylation in the nucleus accumbens in incubation of cocaine craving. J Neurosci. 2015;35:8042–58.
Bertran-Gonzalez J, Bosch C, Maroteaux M, Matamales M, Hervé D, Valjent E, et al. Opposing patterns of signaling activation in dopamine D1 and D2 receptor-expressing striatal neurons in response to cocaine and haloperidol. J Neurosci. 2008;28:5671–85.
Brami‐Cherrier K, Roze E, Girault J-A, Betuing S, Caboche J. Role of the ERK/MSK1 signalling pathway in chromatin remodelling and brain responses to drugs of abuse. J Neurochem. 2009;108:1323–35.
Scobie KN, Damez-Werno D, Sun H, Shao N, Gancarz A, Panganiban CH, et al. Essential role of poly(ADP-ribosyl)ation in cocaine action. Proc Natl Acad Sci USA. 2014;111:2005–10.
Lepack AE, Werner CT, Stewart AF, Fulton SL, Zhong P, Farrelly LA, et al. Dopaminylation of histone H3 in ventral tegmental area regulates cocaine seeking. Science. 2020;368:197–201.
Sun H, Maze I, Dietz DM, Scobie KN, Kennedy PJ, Damez-Werno D, et al. Morphine epigenomically regulates behavior through alterations in histone H3 lysine 9 dimethylation in the nucleus accumbens. J Neurosci. 2012;32:17454–64.
Maze I, Feng J, Wilkinson MB, Sun H, Shen L, Nestler EJ. Cocaine dynamically regulates heterochromatin and repetitive element unsilencing in nucleus accumbens. Proc Natl Acad Sci USA. 2011;108:3035–40.
Liu XS, Wu H, Ji X, Stelzer Y, Wu X, Czauderna S, et al. Editing DNA methylation in the mammalian genome. Cell. 2016;167:233–247.e17.
Liao H-K, Hatanaka F, Araoka T, Reddy P, Wu MZ, Sui Y, et al. In vivo target gene activation via CRISPR/Cas9-mediated trans-epigenetic modulation. Cell. 2017;171:1495–1507.e15.
Heller EA, Cates HM, Peña CJ, Sun H, Shao N, Feng J, et al. Locus-specific epigenetic remodeling controls addiction- and depression-related behaviors. Nat. Neurosci. 2014;17:1720–7.
Heller EA, Hamilton PJ, Burek DD, Lombroso SI, Peña CJ, Neve RL, et al. Targeted epigenetic remodeling of the Cdk5 gene in nucleus accumbens regulates cocaine- and stress-evoked behavior. J Neurosci. 2016;36:4690–7.
Monsey MS, Ota KT, Akingbade IF, Hong ES, Schafe GE. Epigenetic alterations are critical for fear memory consolidation and synaptic plasticity in the lateral amygdala. PLoS ONE. 2011;6:e19958.
Massart R, Freyburger M, Suderman M, Paquet J, El Helou J, Belanger-Nelson E, et al. The genome-wide landscape of DNA methylation and hydroxymethylation in response to sleep deprivation impacts on synaptic plasticity genes. Transl Psychiatry. 2014;4:e347–e347.
Kyzar EJ, Pandey SC. Molecular mechanisms of synaptic remodeling in alcoholism. Neurosci Lett. 2015;601:11–19.
Rogge GA, Wood MA. The role of histone acetylation in cocaine-induced neural plasticity and behavior. Neuropsychopharmacology. 2013;38:94–110.
Kyzar EJ, Floreani C, Teppen TL & Pandey SC. Adolescent alcohol exposure: burden of epigenetic reprogramming, synaptic remodeling, and adult psychopathology. Front. Neurosci. 2016;10:222.
Maze I, Covington HE, Dietz DM, LaPlant Q, Renthal W, Russo SJ, et al. Essential role of the histone methyltransferase G9a in cocaine-induced plasticity. Science. 2010;327:213–6.
Robison AJ, Nestler EJ. Transcriptional and epigenetic mechanisms of addiction. Nat Rev Neurosci. 2011;12:623–37.
Lobo MK, Zaman S, Damez-Werno DM, Koo JW, Bagot RC, DiNieri JA, et al. ΔFosB induction in striatal medium spiny neuron subtypes in response to chronic pharmacological, emotional, and optogenetic stimuli. J Neurosci. 2013;33:18381–95.
Huang YH, Lin Y, Brown TE, Han MH, Saal DB, Neve RL, et al. CREB modulates excitability of nucleus accumbens neurons. Nat Neurosci. 2006;9:475–7.
Murphy DD, Segal M. Morphological plasticity of dendritic spines in central neurons is mediated by activation of cAMP response element binding protein. Proc Natl Acad Sci USA. 1997;94:1482–7.
Grueter BA, Robison AJ, Neve RL, Nestler EJ, Malenka RC. ∆FosB differentially modulates nucleus accumbens direct and indirect pathway function. Proc Natl Acad Sci USA. 2013;110:1923–8.
Smith ACW, Kenny PJ. MicroRNAs regulate synaptic plasticity underlying drug addiction. Genes Brain Behav. 2018;17:e12424.
Nudelman AS, DiRocco DP, Lambert TJ, Garelick MG, Le J, Nathanson NM, et al. Neuronal activity rapidly induces transcription of the CREB-regulated microRNA-132, in vivo. Hippocampus. 2010;20:492–8.
CAS PubMed PubMed Central Google Scholar
Yasui DH, Peddada S, Bieda MC, Vallero RO, Hogart A, Nagarajan RP, et al. Integrated epigenomic analyses of neuronal MeCP2 reveal a role for long-range interaction with active genes. Proc Natl Acad Sci USA. 2007;104:19416–21.
Chahrour M, Jung SY, Shaw C, Zhou X, Wong ST, Qin J, et al. MeCP2, a key contributor to neurological disease, activates and represses transcription. Science. 2008;320:1224–9.
De Crescenzo F, Ciabattini M, D'Alò GL, De Giorgi R, Del Giovane C, Cassar C, et al. Comparative efficacy and acceptability of psychosocial interventions for individuals with cocaine and amphetamine addiction: a systematic review and network meta-analysis. PLOS Med. 2018;15:e1002715.
Phillips KA, Epstein DH, Preston KL. Psychostimulant addiction treatment. Neuropharmacology. 2014;87:150–60.
Mattick RP, Breen C, Kimber J & Davoli M. Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane Database Syst. Rev. 2009;CD002209. https://doi.org/10.1002/14651858.CD002209.pub2 .
Hartmann‐Boyce J, Chepkin SC, Ye W, Bullen C & Lancaster T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst Rev. 2018. https://doi.org/10.1002/14651858.CD000146.pub5 .
Tardelli VS, Bisaga A, Arcadepani FB, Gerra G, Levin FR, Fidalgo TM. Prescription psychostimulants for the treatment of stimulant use disorder: a systematic review and meta-analysis. Psychopharmacology. 2020;237:2233–55.
Darke S & Farrell M. Which medications are suitable for agonist drug maintenance? Addiction. 2016;111:767–74.
Kosten TR, Domingo CB, Shorter D, Orson F, Green C, Somoza E, et al. Vaccine for cocaine dependence: a randomized double-blind placebo-controlled efficacy trial. Drug Alcohol Depend. 2014;140:42–47.
Hossain MK, Hassanzadeganroudsari M, Nurgali K, Apostolopoulos V. Vaccine development against methamphetamine drug addiction. Expert Rev Vaccines. 2020;19:1105–14.
Dackis C, O’Brien C. Neurobiology of addiction: treatment and public policy ramifications. Nat Neurosci. 2005;8:1431–6.
Benabid AL, Pollak P, Gervason C, Hoffmann D, Gao DM, Hommel M, et al. Long-term suppression of tremor by chronic stimulation of the ventral intermediate thalamic nucleus. Lancet. 1991;337:403–6.
Bergman H, Wichmann T, DeLong MR. Reversal of experimental parkinsonism by lesions of the subthalamic nucleus. Science. 1990;249:1436–8.
Limousin P, Pollak P, Benazzouz A, Hoffmann D, Le Bas JF, Broussolle E, et al. Effect on parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet. 1995;345:91–95.
Johansen-Berg H, Gutman DA, Behrens TE, Matthews PM, Rushworth MF, Katz E, et al. Anatomical connectivity of the subgenual cingulate region targeted with deep brain stimulation for treatment-resistant depression. Cereb Cortex. 2008;1991:1374–83.
Greenberg BD, Malone DA, Friehs GM, Rezai AR, Kubu CS, Malloy PF, et al. Three-year outcomes in deep brain stimulation for highly resistant obsessive-compulsive disorder. Neuropsychopharmacology. 2006;31:2384–93.
Porta M, Brambilla A, Cavanna AE, Servello D, Sassi M, Rickards H, et al. Thalamic deep brain stimulation for treatment-refractory Tourette syndrome: two-year outcome. Neurology. 2009;73:1375–80.
Kuhn J, Lenartz D, Huff W, Lee S, Koulousakis A, Klosterkoetter J, et al. Remission of alcohol dependency following deep brain stimulation of the nucleus accumbens: valuable therapeutic implications? J Neurol Neurosurg Psychiatry. 2007;78:1152–3.
Mantione M, van de Brink W, Schuurman PR, Denys D. Smoking cessation and weight loss after chronic deep brain stimulation of the nucleus accumbens: therapeutic and research implications: case report. Neurosurgery. 2010;66:E218.
Levy D, Shabat-Simon M, Shalev U, Barnea-Ygael N, Cooper A, Zangen A. Repeated electrical stimulation of reward-related brain regions affects cocaine but not “natural” reinforcement. J Neurosci. 2007;27:14179–89.
Liu H-Y, Jin J, Tang JS, Sun WX, Jia H, Yang XP, et al. Chronic deep brain stimulation in the rat nucleus accumbens and its effect on morphine reinforcement. Addict Biol. 2008;13:40–46.
Vassoler FM, Schmidt HD, Gerard ME, Famous KR, Ciraulo DA, Kornetsky C, et al. Deep brain stimulation of the nucleus accumbens shell attenuates cocaine priming-induced reinstatement of drug seeking in rats. J Neurosci. 2008;28:8735–9.
Batra V, Tran TL, Caputo J, Guerin GF, Goeders NE, Wilden J. Intermittent bilateral deep brain stimulation of the nucleus accumbens shell reduces intravenous methamphetamine intake and seeking in Wistar rats. J Neurosurg. 2017;126:1339–50.
Heinze H-J, et al. Counteracting incentive sensitization in severe alcohol dependence using deep brain stimulation of the nucleus accumbens: clinical and basic science aspects. Front Hum Neurosci. 2009;3:22.
Kuhn J, Gründler TO, Bauer R, Huff W, Fischer AG, Lenartz D, et al. Successful deep brain stimulation of the nucleus accumbens in severe alcohol dependence is associated with changed performance monitoring. Addict Biol. 2011;16:620–3.
Kuhn J, Möller M, Treppmann JF, Bartsch C, Lenartz D, Gruendler TO, et al. Deep brain stimulation of the nucleus accumbens and its usefulness in severe opioid addiction. Mol Psychiatry. 2014;19:145–6.
Valencia-Alfonso C-E, Luigjes J, Smolders R, Cohen MX, Levar N, Mazaheri A, et al. Effective deep brain stimulation in heroin addiction: a case report with complementary intracranial electroencephalogram. Biol Psychiatry. 2012;71:e35–37.
Voges J, Müller U, Bogerts B, Münte T, Heinze H-J. Deep brain stimulation surgery for alcohol addiction. World Neurosurg. 2013;80:S28.e21–31.
Wang TR, Moosa S, Dallapiazza RF, Elias WJ, Lynch WJ. Deep brain stimulation for the treatment of drug addiction. Neurosurg Focus. 2018;45:E11.
Sanna A, Fattore L, Badas P, Corona G, Diana M. The hypodopaminergic state ten years after: transcranial magnetic stimulation as a tool to test the dopamine hypothesis of drug addiction. Curr Opin Pharmacol. 2021;56:61–67.
Verrico CD, Haile CN, Newton TF, Kosten TR, Garza RDL. Pharmacotherapeutics for substance-use disorders: a focus on dopaminergic medications. Expert Opin Investig Drugs. 2013;22:1549–68.
Amiaz R, Levy D, Vainiger D, Grunhaus L, Zangen A. Repeated high-frequency transcranial magnetic stimulation over the dorsolateral prefrontal cortex reduces cigarette craving and consumption. Addiction. 2009;104:653–60.
Pettorruso M, Di Giuda D, Martinotti G, Cocciolillo F, De Risio L, Montemitro C, et al. Dopaminergic and clinical correlates of high-frequency repetitive transcranial magnetic stimulation in gambling addiction: a SPECT case study. Addict Behav. 2019;93:246–9.
Cho SS, Strafella AP. rTMS of the left dorsolateral prefrontal cortex modulates dopamine release in the ipsilateral anterior cingulate cortex and orbitofrontal cortex. PLoS ONE. 2009;4:e6725.
Strafella AP, Paus T, Fraraccio M, Dagher A. Striatal dopamine release induced by repetitive transcranial magnetic stimulation of the human motor cortex. Brain. 2003;126:2609–15.
Ekhtiari H, Tavakoli H, Addolorato G, Baeken C, Bonci A, Campanella S, et al. Transcranial electrical and magnetic stimulation (tES and TMS) for addiction medicine: a consensus paper on the present state of the science and the road ahead. Neurosci Biobehav Rev. 2019;104:118–40.
Wu X-Q, Zan GY, Ju YY, Chen TZ, Guo LB, Jiao DL, et al. Low-frequency repetitive transcranial magnetic stimulation inhibits the development of methamphetamine-induced conditioned place preference. Behav Brain Res. 2018;353:129–36.
Dackis CA, Kampman KM, Lynch KG, Plebani JG, Pettinati HM, Sparkman T, et al. A double-blind, placebo-controlled trial of modafinil for cocaine dependence. J Subst Abus Treat. 2012;43:303–12.
Shearer J, Darke S, Rodgers C, Slade T, van Beek I, Lewis J, et al. A double-blind, placebo-controlled trial of modafinil (200 mg/day) for methamphetamine dependence. Addiction. 2009;104:224–33.
Chiamulera C, Piva A, Abraham WC. Glutamate receptors and metaplasticity in addiction. Curr Opin Pharmacol. 2021;56:39–45.
Le Moal M, Koob GF. Drug addiction: pathways to the disease and pathophysiological perspectives. Eur Neuropsychopharmacol. 2007;17:377–93.
Luigjes J, Segrave R, de Joode N, Figee M, Denys D. Efficacy of invasive and non-invasive brain modulation interventions for addiction. Neuropsychol Rev. 2019;29:116–38.
Jordi E, Heiman M, Marion-Poll L, Guermonprez P, Cheng SK, Nairn AC, Greengard P, Girault J-A. Proceedings of the National Academy of Sciences . 2013;110:9511-16. https://doi.org/10.1073/pnas.1307116110 .
Wang H, Wang L, Erdjument-Bromage H, Vidal M, Tempst P, Jones RS, et al. Role of histone H2A ubiquitination in Polycomb silencing. Nature. 2004;431:873–8.
Download references
Acknowledgements
We thank Michele Zoli, Romain Icick and Daniel Rial for helpful comments and corrections on the manuscript. Julian Cheron is supported by a fellowship of the FRS-FNRS (Belgium). Alban de Kerchove d´Exaerde is a Research Director of the FRS-FNRS. FRS-FNRS (Belgium). Fondation Simone et Pierre Clerdent, Fondation ULB, supported this study.
Author information
Authors and affiliations.
Laboratory of Neurophysiology, ULB Neuroscience Institute, Université Libre de Bruxelles (ULB), Brussels, B-1070, Belgium
Julian Cheron & Alban de Kerchove d’Exaerde
You can also search for this author in PubMed Google Scholar
Contributions
JC and AKE wrote the paper and AKE supervised all the work.
Corresponding author
Correspondence to Alban de Kerchove d’Exaerde .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Cheron, J., Kerchove d’Exaerde, A.d. Drug addiction: from bench to bedside. Transl Psychiatry 11 , 424 (2021). https://doi.org/10.1038/s41398-021-01542-0
Download citation
Received : 05 April 2021
Revised : 14 July 2021
Accepted : 23 July 2021
Published : 12 August 2021
DOI : https://doi.org/10.1038/s41398-021-01542-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Snp-based and haplotype-based genome-wide association on drug dependence in han chinese.
- Yangyang Liu
BMC Genomics (2024)
Unraveling Relapse in Male Forensic Psychiatric Patients with Substance Use Disorders—The Impact of Social, Psychiatric, and Personality Factors Post Long-Term Remission
- Michael Fritz
- Felipe Montiel
- Judith Streb
International Journal of Mental Health and Addiction (2024)
USP7/Maged1-mediated H2A monoubiquitination in the paraventricular thalamus: an epigenetic mechanism involved in cocaine use disorder
- Julian Cheron
- Leonardo Beccari
- Alban de Kerchove d’Exaerde
Nature Communications (2023)
Methylation and expression quantitative trait locus rs6296 in the HTR1B gene is associated with susceptibility to opioid use disorder
- Jianbo Zhang
Psychopharmacology (2022)
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies


An official website of the United States government
Here’s how you know
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you’ve safely connected to the .gov website. Share sensitive information only on official, secure websites.
Drugs, Brains, and Behavior: The Science of Addiction Preface
How science has revolutionized the understanding of drug addiction.
For much of the past century, scientists studying drugs and drug use labored in the shadows of powerful myths and misconceptions about the nature of addiction. When scientists began to study addictive behavior in the 1930s, people with an addiction were thought to be morally flawed and lacking in willpower. Those views shaped society’s responses to drug use, treating it as a moral failing rather than a health problem, which led to an emphasis on punishment rather than prevention and treatment.
Today, thanks to science, our views and our responses to addiction and the broader spectrum of substance use disorders have changed dramatically. Groundbreaking discoveries about the brain have revolutionized our understanding of compulsive drug use, enabling us to respond effectively to the problem.
As a result of scientific research, we know that addiction is a medical disorder that affects the brain and changes behavior. We have identified many of the biological and environmental risk factors and are beginning to search for the genetic variations that contribute to the development and progression of the disorder. Scientists use this knowledge to develop effective prevention and treatment approaches that reduce the toll drug use takes on individuals, families, and communities.
Despite these advances, we still do not fully understand why some people develop an addiction to drugs or how drugs change the brain to foster compulsive drug use. This booklet aims to fill that knowledge gap by providing scientific information about the disorder of drug addiction, including the many harmful consequences of drug use and the basic approaches that have been developed to prevent and treat substance use disorders.
At the National Institute on Drug Abuse (NIDA), we believe that increased understanding of the basics of addiction will empower people to make informed choices in their own lives, adopt science-based policies and programs that reduce drug use and addiction in their communities, and support scientific research that improves the Nation’s well-being.
Nora D. Volkow, M.D. Director National Institute on Drug Abuse
Warning: The NCBI web site requires JavaScript to function. more...

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Substance Abuse and Mental Health Services Administration (US); Office of the Surgeon General (US). Facing Addiction in America: The Surgeon General's Report on Alcohol, Drugs, and Health [Internet]. Washington (DC): US Department of Health and Human Services; 2016 Nov.

Facing Addiction in America: The Surgeon General's Report on Alcohol, Drugs, and Health [Internet].
Chapter 1 introduction and overview of the report.
- Chapter 1 Preview
The United States has a serious substance misuse problem. Substance misuse is the use of alcohol or drugs in a manner, situation, amount, or frequency that could cause harm to the user or to those around them. Alcohol and drug misuse and related substance use disorders affect millions of Americans and impose enormous costs on our society. In 2015, 66.7 million people in the United States reported binge drinking in the past month and 27.1 million people were current users of illicit drugs or misused prescription drugs. 3 The accumulated costs to the individual, the family, and the community are staggering and arise as a consequence of many direct and indirect effects, including compromised physical and mental health, increased spread of infectious disease, loss of productivity, reduced quality of life, increased crime and violence, increased motor vehicle crashes, abuse and neglect of children, and health care costs.
The most devastating consequences are seen in the tens of thousands of lives that are lost each year as a result of substance misuse. Alcohol misuse contributes to 88,000 deaths in the United States each year; 1 in 10 deaths among working adults are due to alcohol misuse. 6 In addition, in 2014 there were 47,055 drug overdose deaths including 28,647 people who died from a drug overdose involving some type of opioid, including prescription pain relievers and heroin—more than in any previous year on record. 7
Even though the United States spends more than any other country on health care, it ranks 27 th in life expectancy, which has plateaued or decreased for some segments of the population at a time when life expectancy continues to increase in other developed countries—and the difference is largely due to substance misuse and associated physical and mental health problems. For example, recent research has shown an unprecedented increase in mortality among middle-aged White Americans between 1999 and 2014 that was largely driven by alcohol and drug misuse and suicides, although this trend was not seen within other racial and ethnic populations such as Blacks and Hispanics. 8 An analysis from the Centers for Disease Control and Prevention (CDC) demonstrated that alcohol and drug misuse accounted for a roughly 4-month decline in life expectancy among White Americans; no other cause of death had a larger negative impact in this population. 9
Substance misuse and substance use disorders also have serious economic consequences, costing more than $400 billion annually in crime, health, and lost productivity. 10 , 11 These costs are of a similar order of magnitude to those associated with other serious health problems such as diabetes, which is estimated to cost the United States $245 billion each year. 12 Alcohol misuse and alcohol use disorders alone costs the United States approximately $249 billion in lost productivity, health care expenses, law enforcement, and other criminal justice costs. 10 The costs associated with drug use disorders and use of illegal drugs and non-prescribed medications were estimated to be more than $193 billion in 2007. 11
Despite decades of expense and effort focused on a criminal justice-based model for addressing substance use-related problems, substance misuse remains a national public health crisis that continues to rob the United States of its most valuable asset: its people. In fact, high annual rates of past-month illicit drug use and binge drinking among people aged 12 years and older from 2002 through 2014 ( Figure 1.1 ) emphasize the importance of implementing evidence-based public-health-focused strategies to prevent and treat alcohol and drug problems in the United States. 13 A public health approach seeks to improve the health and safety of the population by addressing underlying social, environmental, and economic determinants of substance misuse and its consequences, to improve the health, safety, and well-being of the entire population.
Past Month Rates of Substance Use Among People Aged 12 or Older: Percentages, 2002-2014, 2014 National Survey on Drug Use and Health (NSDUH). Notes: The National Survey on Drug Use and Health (NSDUH) obtains information on nine categories of illicit drugs: (more...)
This Surgeon General's Report has been created because of the important health and social problems associated with alcohol and drug misuse in America. As described in this Report , a comprehensive approach is needed to address substance use problems in the United States that includes several key components:
- Enhanced public education to improve awareness about substance use problems and demand for more effective policies and practices to address them;
- Widespread implementation of evidence-based prevention policies and programs to prevent substance misuse and related harms;
- Improved access to evidence-based treatment services, integrated with mainstream health care, for those at risk for or affected by substance use disorders;
- Recovery support services (RSS) to assist individuals in maintaining remission and preventing relapse; and
- Research-informed public policies and financing strategies to ensure that substance misuse and use disorder services are accessible, compassionate, efficient, and sustainable.
The Public Health System . The Public Health System is defined as “all public, private, and voluntary entities that contribute to the delivery of essential public health services within a jurisdiction” and includes state and local public health agencies, public safety agencies, health care providers, human service and charity organizations, recreation and arts-related organizations, economic and philanthropic organizations, and education and youth development organizations. 2
The Health Care System . The World Health Organization defines a health care system as (1) all the activities whose primary purpose is to promote, restore, and/or maintain health, and (2) the people, institutions, and resources, arranged together in accordance with established policies, to improve the health of the population they serve. The health care system is made up of diverse health care organizations ranging from primary care, specialty substance use disorder treatment (including residential and outpatient settings), mental health care, infectious disease clinics, school clinics, community health centers, hospitals, emergency departments, and others. 5
Recognizing these needs, the Report explains the neurobiological basis for substance use disorders and provides the biological, psychological, and social frameworks for improving diagnosis, prevention, and treatment of alcohol and drug misuse. It also describes evidence-based prevention strategies, such as public policies that can reduce substance misuse problems (e.g., driving under the influence [DUI]); effective treatment strategies, including medications and behavioral therapies for treating substance use disorders; and RSS for people who have completed treatment. Additionally, the Report describes recent changes in health care financing, including changes in health insurance regulations, which support the integration of clinical prevention and treatment services for substance use disorders into mainstream health care practice, and defines a research agenda for addressing alcohol and drug misuse as medical conditions.
Thus, this first Surgeon General's Report on Alcohol, Drugs, and Health is not issued simply because of the prevalence of substance misuse or even the related devastating harms and costs, but also to help inform policymakers, health care professionals, and the general public about effective, practical, and sustainable strategies to address these problems. These strategies have the potential to substantially reduce substance misuse and related problems; promote early intervention for substance misuse and substance use disorders; and improve the availability of high-quality treatment and RSS for persons with substance use disorders.
A Public Health Model for Addressing Substance Misuse and Related Consequences
A public health systems approach to substance misuse and its consequences, including substance use disorders, aims to:
- Define the problem through the systematic collection of data on the scope, characteristics, and consequences of substance misuse;
- Identify the risk and protective factors that increase or decrease the risk for substance misuse and its consequences, and the factors that could be modified through interventions;
- Work across the public and private sector to develop and test interventions that address social, environmental, or economic determinants of substance misuse and related health consequences;
- Support broad implementation of effective prevention and treatment interventions and recovery supports in a wide range of settings; and
- Monitor the impact of these interventions on substance misuse and related problems as well as on risk and protective factors.
A healthy community is one with not just a strong health care system but also a strong public health educational system, safe streets, effective public transportation and affordable, high quality food and housing -where all individuals have opportunities to thrive. Thus, community leaders should work together to mobilize the capacities of health care organizations, social service organizations, educational systems, community-based organizations, government health agencies, religious institutions, law enforcement, local businesses, researchers, and other public, private, and voluntary entities that can contribute to the above aims. Everyone has a role to play in addressing substance misuse and its consequences and thereby improving the public health.
- Substances Discussed in this Report
This Report defines a substance as a psychoactive compound with the potential to cause health and social problems, including substance use disorders (and their most severe manifestation, addiction). These substances can be divided into three major categories: Alcohol, Illicit Drugs (a category that includes prescription drugs used nonmedically), and Over-the-Counter Drugs. Some specific examples of the substances included in each of these categories are included in Table 1.1 . Over-the-Counter Drugs are not discussed in this Report , but are included in Appendix D - Important Facts about Alcohol and Drugs.
Categories and Examples of Substances.
Although different in many respects, the substances discussed in this Report share three features that make them important to public health and safety. First, many people use and misuse these substances: 66.7 million individuals in the United States aged 12 or older admitted to binge drinking in the past month and 27.1 million people aged 12 or older used an illicit drug in the past month 3
Second, individuals can use these substances in a manner that causes harm to the user or those around them . This is called substance misuse and often results in health or social problems, referred to in this Report as substance misuse problems. Misuse can be of low severity and temporary, but it can also result in serious, enduring, and costly consequences due to motor vehicle crashes, 18 , 19 intimate partner and sexual violence, 20 child abuse and neglect, 21 suicide attempts and fatalities, 22 overdose deaths, 23 various forms of cancer 24 (e.g., breast cancer in women), 25 heart and liver diseases, 26 HIV/AIDS, 27 and problems related to drinking or using drugs during pregnancy, such as fetal alcohol spectrum disorders (FASDs) or neonatal abstinence syndrome (NAS). 28
Third, prolonged, repeated misuse of any of these substances can produce changes to the brain that can lead to a substance use disorder , an independent illness that significantly impairs health and function and may require specialty treatment Disorders can range from mild to severe. Severe and chronic substance use disorders are commonly referred to as addictions.
FOR MORE ON THIS TOPIC
See the section on Diagnosing a Substance Use Disorder later in this chapter.
Key Terms Used in the Report
Addiction : The most severe form of substance use disorder, associated with compulsive or uncontrolled use of one or more substances. Addiction is a chronic brain disease that has the potential for both recurrence (relapse) and recovery.
Substance : A psychoactive compound with the potential to cause health and social problems, including substance use disorders (and their most severe manifestation, addiction). For a list of substance categories included in this Report see Table 1.1 . Note: Cigarettes and other tobacco products are only briefly discussed here due to extensive coverage in prior Surgeon General's Reports. 14 - 17
Substance Use : The use—even one time—of any of the substances in this Report .
Substance Misuse : The use of any substance in a manner, situation, amount, or frequency that can cause harm to users or to those around them. For some substances or individuals, any use would constitute misuse (e.g., underage drinking, injection drug use).
Binge Drinking : Binge drinking for men is drinking 5 or more standard alcoholic drinks, and for women, 4 or more standard alcoholic drinks on the same occasion on at least 1 day in the past 30 days.
Heavy Drinking : Defined by the CDC as consuming 8 or more drinks per week for women, and 15 or more drinks per week for men, and by the Substance Abuse and Mental Health Services Administration (SAMHSA), for research purposes, as binge drinking on 5 or more days in the past 30 days.
Standard Drink : Based on the 2015-2020 Dietary Guidelines for Americans , a standard drink is defined as shown in the graphic below. All of these drinks contain 14 grams (0.6 ounces) of pure alcohol.

Source: U.S. Department of Health and Human Services and U.S. Department of Agriculture, (2015). 29
Substance Misuse Problems or Consequences : Any health or social problem that results from substance misuse. Substance misuse problems or consequences may affect the substance user or those around them, and they may be acute (e.g., an argument or fight, a motor vehicle crash, an overdose) or chronic (e.g., a long-term substance-related medical, family, or employment problem, or chronic medical condition, such as various cancers, heart disease, and liver disease). These problems may occur at any age and are more likely to occur with greater frequency of substance misuse.
Substance Use Disorder: A medical illness caused by repeated misuse of a substance or substances. According to the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 30 substance use disorders are characterized by clinically significant impairments in health, social function, and impaired control over substance use and are diagnosed through assessing cognitive, behavioral, and psychological symptoms. Substance use disorders range from mild to severe and from temporary to chronic. They typically develop gradually over time with repeated misuse, leading to changes in brain circuits governing incentive salience (the ability of substance-associated cues to trigger substance seeking), reward, stress, and executive functions like decision making and self-control. Multiple factors influence whether and how rapidly a person will develop a substance use disorder. These factors include the substance itself; the genetic vulnerability of the user; and the amount, frequency, and duration of the misuse. Note: A severe substance use disorder is commonly called an addiction.
Relapse : The return to drug use after a significant period of abstinence.
Recovery : A process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential. Even individuals with severe and chronic substance use disorders can, with help, overcome their substance use disorder and regain health and social function. This is called remission. When those positive changes and values become part of a voluntarily adopted lifestyle, that is called “being in recovery.” Although abstinence from all substance misuse is a cardinal feature of a recovery lifestyle, it is not the only healthy, pro-social feature.
- Prevalence of Substance Use, Misuse Problems, and Disorders
How widespread are substance use, misuse, and substance use disorders in the United States? The annual National Survey on Drug Use and Health (NSDUH) gathers data on the scope and prevalence of substance use, misuse, and related disorders, as well as utilization of substance use disorder treatment, among Americans aged 12 and older, representing more than 265 million people. Table 1.2 provides selected findings from the 2015 NSDUH. The table provides only general statistics for the United States as a whole; readers are urged to consult NSDUH's detailed tables 3 for subpopulation estimates.
Past Year Substance Use, Past Year Initiation of Substance Use, and Met Diagnostic Criteria for a Substance Use Disorder in the Past Year Among Persons Aged 12 Years or Older for Specific Substances: Numbers in Millions and Percentages, 2015 National (more...)
Over 175 million persons aged 12 and older (65.7 percent of this population) reported alcohol use in the past year, with over 66 million (24.9 percent) reporting binge drinking in the past month ( Table 1.2 ). More than 36 million (13.5 percent) reported using marijuana in the past year, 12.5 million reported misusing prescription pain relievers, and over 300,000 reported using heroin in the past year. Almost 8 percent of the population met diagnostic criteria for a substance use disorder for alcohol or illicit drugs, and another 1 percent met diagnostic criteria for both an alcohol and illicit drug use disorder. Although 20.8 million people (7.8 percent of the population) met the diagnostic criteria for a substance use disorder in 2015, only 2.2 million individuals (10.4 percent) received any type of treatment. Of those treated, 63.7 percent received treatment in specialty substance use disorder treatment programs. 3
Prevalence . The proportion of a population who have (or had) a specific characteristic—for example, an illness, condition, behavior, or risk factor— in a given time period.
Several specific findings shown in Table 1.2 bear emphasis. Past year misuse of prescription psychotherapeutic drugs was reported by 18.9 million individuals in 2015 (7.1 percent of the population). 3 Within this category, prescribed opioid pain relievers (e.g., OxyContin®, Vicodin®, Lortab®) accounted for 12.5 million people, followed by tranquilizers, such as Xanax®, reported by 6.1 million people; stimulants, such as Adderall® or Ritalin®, reported by 5.3 million people; and sedatives, such as Valium®, reported by 1.5 million people. 3
Substance Use Disorder Treatment Programs
Historically, treatment services were designed for people with severe substance use disorders (addictions), and programs were generally referred to as “specialty addiction treatment programs.” Today, individuals with mild to severe substance use disorders may receive treatment. These treatments are delivered by specialty programs, as well as by more generalist providers (e.g., primary care and general mental health providers). Not everyone with a substance use disorder will need ongoing treatment; many will require only a brief intervention and monitoring. Because treatments vary substantially in level of specialization, content, duration, and setting, and because those receiving services may differ substantially in the severity, duration, and complexity of their substance use disorder, this Report uses the phrase “substance use disorder treatment” as the generic term to capture the broad spectrum of advice, therapies, services, and monitoring provided to the group of individuals with mild to severe substance use disorders. The programs and services that provide specialty treatment are referred to as “substance use disorder treatment programs or services.”
The prevalence of past 30-day use of “any illicit drugs” (a broad category including marijuana/hashish, cocaine/crack, heroin, hallucinogens, inhalants, and prescription psychotherapeutic medications used nonmedically) rose from 9.4 percent in 2013 to 10.2 percent in 2014 among persons aged 12 and older ( Figure 1.2 ). This 2014 prevalence rate for illicit drugs is significantly higher than it was in any year from 2002 to 2013. However, no significant changes were observed that year specifically in the use of prescription psychotherapeutic drugs, cocaine, or hallucinogens, suggesting that the observed increase was primarily related to increased use of marijuana. Marijuana was the most frequently used illicit drug (35.1 million past year users). 31 The rate for past month marijuana use in 2014 was significantly higher than it was in any year from 2002 to 2013, with the prevalence of past 30-day marijuana use rising from 7.5 percent in 2013 to 8.4 percent in 2014. 13 (Note: In 2015, changes were made to the NSDUH questionnaire and data collection procedures that do not allow for the presentation of trend data beyond 2014. For more information, see Summary of the Effects of the 2015 NSDUH Questionnaire Redesign: Implications for Data Users . 32 )
Trends in Binge Drinking and Past 30-Day Use of Illicit Drugs among Persons Aged 12 Years or Older, 2014 National Survey on Drug Use and Health (NSDUH). Notes: * Difference between this estimate and the 2014 estimate is statistically significant at the (more...)
Demographics of Substance Use
Table 1.3 and Table 1.4 show substance use by demographic characteristics. Prevalence of substance misuse and substance use disorders differs by race and ethnicity and gender, and these factors can also influence access to health care and substance use disorder treatment. Past year alcohol use for men was 68.6 percent and for women it was 62.9 percent. Past month binge alcohol use was 29.6 percent for men and 20.5 percent for women. The prevalence of past month binge alcohol use was 24.1 percent for American Indians or Alaska Natives, 25.7 percent for Hispanics or Latinos, and 26.0 for Whites. Prevalence of an alcohol use disorder was 7.8 percent for men and 4.1 percent for women. The prevalence of an illicit drug use disorder was 3.8 percent for men and 2.0 percent for women.
Past Year Alcohol Use, Past Month Binge Alcohol Use, and Met Diagnostic Criteria for a Substance Use Disorder in the Past Year Among Persons Aged 12 Years or Older: Numbers in Millions and Percentages, 2015 National Survey on Drug Use and Health (NSDUH). (more...)
Past Year Substance Use, Past 30-Day Illicit Drug Use, and Met Diagnostic Criteria for a Substance Use Disorder in the Past Year Among Persons Aged 12 Years or Older: Numbers in Millions and Percentages, 2015 National Survey on Drug Use and Health (NSDUH). (more...)
Relevance of Substance Use and Misuse
It is sometimes thought that concern over substance use and misuse should be secondary to the real issue of substance use disorders and especially their severest manifestation, addiction, which has captured media headlines and has been linked to many health and social problems. This is an important misconception. Individuals with substance use disorders have elevated rates of substance misuse–related health and social problems and costs, but as shown in the last columns of Table 1.2 , Table 1.3 , and Table 1.4 , many people who misuse substances do not meet the diagnostic criteria for a substance use disorder. For example, binge drinking at least once during the past month was self-reported by over 66 million individuals. By definition, those episodes have the potential for producing harm to the user and/or to those around them, through increases in motor vehicle crashes, violence, and alcohol-poisonings. 33 Similarly, in 2015, 12.5 million individuals misused a pain reliever in the past year—setting the stage for a potential overdose—but only 2.9 million met diagnostic criteria for a prescription medication disorder. 3
The clear implications of these data are that a comprehensive approach to reducing the misuse of alcohol and drugs—one that includes the implementation of effective prevention programs and policy strategies as well as high-quality treatment services—is needed to reduce the problems and costs of substance misuse in the United States. In fact, greater impact is likely to be achieved by reducing substance misuse in the general population—that is, among people who are not addicted—than among those with severe substance use problems. Of course, efforts to reduce general population rates of substance use and misuse are also likely to reduce rates of substance use disorders, because substance use disorders typically develop over time following repeated episodes of misuse (often at escalating rates) that result in the progressive changes to brain circuitry that underlie addiction.
See Chapter 2 - The Neurobiology of Substance Use , Misuse, and Addiction .
- Costs and Impact of Substance Use and Misuse
Alcohol misuse, illicit drug use, misuse of medications, and substance use disorders are estimated to cost the United States more than $400 billion in lost workplace productivity (in part, due to premature mortality), health care expenses, law enforcement and other criminal justice costs (e.g., drug-related crimes), and losses from motor vehicle crashes. 10 , 11 Furthermore, about three quarters of the costs associated with alcohol use were due to binge drinking, and about 40 percent of those costs were paid by government, emphasizing the huge cost of alcohol misuse to taxpayers. 34
These costs are not unique to the United States. A 2010 study examined the global burden of disability attributable to substance misuse problems and disorders, focusing particularly on lost ability to work and years of life lost to premature mortality. Costs were calculated for 20 age groups and both sexes in 187 countries. 35 Mental and substance use disorders were the leading causes of years lived with disability worldwide, largely because these problems strike individuals early in their lives and can continue—especially if untreated—for long periods.
In addition to the costs to society, substance misuse can have many direct and indirect health and personal consequences for individuals. The direct effects on the user depend on the specific substances used, how much and how often they are used, how they are taken (e.g., orally vs. injected), and other factors. Acute effects can range from changes in mood and basic body functions, such as heart rate or blood pressure, to overdose and death. Alcohol misuse and drug use can also have long-term effects on physical and mental health and can lead to substance use disorders. For example, drug use is associated with chronic pain conditions and cardiovascular and cardiopulmonary diseases. 36 , 37 Alcohol misuse is associated with liver and pancreatic diseases, hypertension, reproductive system disorders, trauma, stroke, FASD, and cancers of the oral cavity, esophagus, larynx, pharynx, liver, colon, and rectum. 26 , 28 For breast cancer, studies have shown that even moderate drinking may increase the risk. 25 Although alcohol consumption is associated with adverse health effects as noted above, the 2015-2020 Dietary Guidelines for Americans indicate that moderate alcohol use can be part of a healthy diet, but only when used by adults of legal drinking age. i
In addition, alcohol and drug use by pregnant women can have profound effects on the developing fetus. Alcohol use during pregnancy can lead to a wide range of disabilities in children, the most severe of which is FASD, characterized by intellectual disabilities, speech and language delays, poor social skills, and sometimes facial deformities. Use of drugs, such as opioids during pregnancy, can result in NAS, a drug-withdrawal syndrome requiring medical intervention and extended hospital stay for newborns. Use of some drugs, such as cocaine, during pregnancy may also lead to premature birth or miscarriage. In addition, substance use during pregnancy may interfere with a child's brain development and result in later consequences for mental functioning and behavior.
Substance misuse also can affect a user's nutrition and sleep, as well as increase the risk for trauma, violence, injury, and contraction of communicable diseases, such as HIV/AIDS and Hepatitis C. These consequences can all contribute to the spectrum of public health consequences of substance misuse and need to be considered both independently and collectively when developing and implementing clinical and public health interventions.
Substance misuse problems can also result in other serious and sometimes fatal health problems and extraordinary costs; they may also lead to unexpected death from other causes. Three examples of these serious, sometimes lethal, problems related to substance misuse are highlighted below.
Driving Under the Influence
In 2014, 9,967 people were killed in motor vehicle crashes while driving under the influence of alcohol, representing nearly one third (31 percent) of all traffic-related fatalities in the United States. 38 DUI continues to be among the most frequent causes for arrests every year. 39 But at approximately 1.3 million per year, these arrests represent only about 1 percent of the actual alcohol-impaired driving incidents reported in national surveys, suggesting that there are many more people who drive while impaired that have not been arrested, putting themselves and others at high risk of being harmed. 18 , 40 In addition to the deaths that result from DUI, the National Highway Traffic Safety Administration (NHTSA) estimates that DUI costs the United States more than $44 billion each year in prosecution, higher insurance rates, higher taxes, medical claims, and property damage. 41
As important as they are, these statistics account for only alcohol-related driving impairment and fail to measure other impairing substances. A study by NHTSA tested oral fluid and blood specimens from a random sample of drivers at the roadside (during daytime on Friday or nighttime Friday to Sunday) and found 12 to 15 percent had used one or more illegal substances. 42 Drivers tested positive for drugs in approximately 16 percent of all motor vehicle crashes. 43
Overdose Deaths
Overdose deaths are typically caused by consuming substances at high intensity and/or by consuming combinations of substances such as alcohol, sedatives, tranquilizers, and opioid pain relievers to the point where critical areas in the brain that control breathing, heart rate, and body temperature stop functioning.
Alcohol Overdose (Alcohol Poisoning)
The CDC reports more than 2,200 alcohol overdose deaths in the United States each year—an average of six deaths every day 44 More than three quarters (76 percent) of alcohol overdose deaths occur among adults between ages 35 and 64, and 76 percent of those who die from alcohol overdose are men.
Drug Overdose (Illicit and Prescription Drugs)
Opioid analgesic pain relievers are now the most prescribed class of medications in the United States, with more than 289 million prescriptions written each year. 45 , 46 The increase in prescriptions of opioid pain relievers has been accompanied by dramatic increases in misuse ( Table 1.1 ) and by a more than 200 percent increase in the number of emergency department visits from 2005 to 2011. 47 In 2014, 47,055 drug overdose deaths occurred in the United States, and 61 percent of these deaths were the result of opioid use, including prescription opioids and heroin. 7 Heroin overdoses have more than tripled from 2010 to 2014. 7 Heroin overdoses were more than five times higher in 2014 (10,574) then ten years before in 2004 (1,878). Additionally, rates of cocaine overdose were higher in 2014 than in the previous six years (5,415 deaths from cocaine overdose). In 2014, there were 17,465 overdoses from illicit drugs and 25,760 overdoses from prescription drugs. 48 Drug overdose deaths also occur as a result of the illicit manufacturing and distribution of synthetic opioids, such as fentanyl, and the illegal diversion of prescription opioids. Illicit fentanyl, for example, is often combined with heroin or counterfeit prescription drugs or sold as heroin, and may be contributing to recent increases in drug overdose deaths. 7 , 49
KEY CONCEPT
The Opioid Crisis. Over-prescription of powerful opioid pain relievers beginning in the 1990s led to a rapid escalation of use and misuse of these substances by a broad demographic of men and women across the country. 1 This led to a resurgence of heroin use, as some users transitioned to using this cheaper street cousin of expensive prescription opioids. As a result, the number of people dying from opioid overdoses soared—increasing nearly four-fold between 1999 and 2014. 4
Intimate Partner Violence, Sexual Assault, and Rape
Intimate partner violence, sexual assault, and rape are crimes with long-lasting effects on victims and great cost to society. 50 , 51 These crimes happen to both women and men and are often associated with substance use. A recent national survey found that 22 percent of women and 14 percent of men reported experiencing severe physical violence from an intimate partner in their lifetimes. 52 In this survey, 19.3 percent of women and 1.7 percent of men reported being raped in their lifetimes, while 43.9 percent of women and 23.4 percent of men reported some other form of sexual violence in their lifetimes. 52 Substance misuse is often related to these crimes.
Numerous studies have found a high correlation between substance use and intimate partner violence, 53 - 56 although this does not mean that substance use causes intimate partner violence. In addition to evidence from the criminal justice arena, recent systematic reviews have found that substance use is both a risk factor for and a consequence of intimate partner violence. 57 - 59
A recent survey of sexual assault and sexual misconduct on college campuses found that use of alcohol and drugs are important risk factors for nonconsensual sexual contact among undergraduate, graduate, and professional students. 20 It is clear that substance use and intimate partner violence and sexual assault are closely linked; however, more research is needed on the nature of the relationship between substance use and these forms of violence to determine how substance use contributes to the perpetration of violence and victimization and how violence contributes to subsequent substance use among both perpetrators and victims.
- Vulnerability to Substance Misuse Problems and Disorders
Risk and Protective Factors: Keys to Vulnerability
Substance misuse problems and substance use disorders are not inevitable. An individual's vulnerability may be partly predicted by assessing the nature and number of their community, caregiver/family, and individual-level risk and protective factors.
Significant community-level risk factors for substance misuse and use disorders include easy access to inexpensive alcohol and other substances. Caregiver/family-level risk factors include low parental monitoring, a family history of substance use or mental disorders, and high levels of family conflict or violence. At the individual level, major risk factors include current mental disorders, low involvement in school, a history of abuse and neglect, and a history of substance use during adolescence, among others. 60
See Chapter 3 - Prevention Programs and Policies .
Community-level protective factors include higher cost for alcohol and other drugs (often achieved by increasing taxes on these products); regulating the number and concentration of retailers selling various substances (e.g., density of alcohol outlets or marijuana dispensaries); preventing illegal alcohol and other drug sales by enforcing existing laws and holding retailers accountable for harms caused by illegal sales (e.g., commercial host [dram shop] liability); availability of healthy recreational and social activities; and other population-level policies and their enforcement. 61 Caregiver/family-level protective factors include support and regular monitoring by parents. 60 Some important individual-level protective factors include involvement in school, engagement in healthy recreational and social activities, and good coping skills. 60
Three important points about vulnerability should be highlighted. First, no single individual or community-level factor determines whether an individual will develop a substance misuse problem or disorder. Second, most risk and protective factors can be modified through preventive programs and policies to reduce vulnerability. Third, although substance misuse problems and disorders may occur at any age, adolescence and young adulthood are particularly critical at-risk periods. Research now indicates that the majority of those who meet criteria for a substance use disorder in their lifetime started using substances during adolescence and met the criteria by age 20 to 25. 62 - 64 One likely reason for this vulnerability in adolescence and young adulthood is that alcohol and other substances have particularly potent effects on developing brain circuits, and recent scientific findings indicate that brain development is not complete until approximately age 21 to 23 in women and 23 to 25 in men. 65 - 67 Among the last brain regions to reach maturity is the prefrontal cortex, the brain region primarily responsible for “adult” abilities, such as delay of reward, extended reasoning, and impulse control. This area of the brain is one of the most affected regions in a substance use disorder.
Substance misuse can begin at any age. Therefore, it is important to focus on prevention of substance misuse across the lifespan as well as the prevention of substance use disorders.
- Diagnosing a Substance Use Disorder
Changes in Understanding and Diagnosis of Substance Use Disorders
Repeated, regular misuse of any of the substances listed in Figure 1.2 may lead to the development of a substance use disorder. Severe substance use disorders are characterized by compulsive use of substance(s) and impaired control of substance use. Substance use disorder diagnoses are based on criteria specified in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM). Much of the substance use disorder data included in this Report is based on definitions included in the DSM-IV, which described two distinct disorders: substance abuse and substance dependence, with specific diagnostic criteria for each. Anyone meeting one or more of the abuse criteria—which focused largely on the negative consequences associated with substance misuse, such as being unable to fulfill family or work obligations, experiencing legal trouble, or engaging in hazardous behavior as a result of drug use—would receive the “abuse” diagnosis. Anyone with three or more of the dependence criteria, which included symptoms of drug tolerance, withdrawal, escalating and uncontrolled substance use, and the use of the substance to the exclusion of other activities, would receive the “dependence” diagnosis. Notably, addiction is not listed as a formal diagnosis in the DSM. However, substance dependence was often used interchangeably with addiction, and tolerance and withdrawal were considered, by many, cardinal features of addiction.
Misuse versus Abuse. This Report uses the term substance misuse, a term that is roughly equivalent to substance abuse. Substance abuse, an older diagnostic term, was defined as use that is unsafe (e.g., drunk or drugged driving), use that leads a person to fail to fulfill responsibilities or gets them in legal trouble, or use that continues despite causing persistent interpersonal problems like fights with a spouse.
However, “substance abuse” is increasingly avoided by professionals because it can be shaming. Instead, substance misuse is now the preferred term. Although misuse is not a diagnostic term, it generally suggests use in a manner that could cause harm to the user or those around them.
The DSM-5, which is the fifth and current version of the DSM, integrates the two DSM-IV disorders, substance abuse and substance dependence, into a single disorder called substance use disorder with mild, moderate , and severe sub-classifications. Individuals are evaluated for a substance use disorder based on 10 or 11 (depending on the substance) equally weighted diagnostic criteria ( Table 1.5 ). Most of these overlap with those used to diagnose DSM-IV dependence and abuse. Individuals exhibiting fewer than two of the symptoms are not considered to have a substance use disorder. Those exhibiting two or three symptoms are considered to have a “mild” disorder, four or five symptoms constitutes a “moderate” disorder, and six or more symptoms is considered a “severe” substance use disorder. 30 In this Report , addiction is used to refer to substance use disorders at the severe end of the spectrum and are characterized by compulsive substance use and impaired control over use.
Criteria for Diagnosing Substance Use Disorders.
Tolerance . Alteration of the body's responsiveness to alcohol or a drug such that higher doses are required to produce the same effect achieved during initial use.
Withdrawal . A set of symptoms that are experienced when discontinuing use of a substance to which a person has become dependent or addicted, which can include negative emotions such as stress, anxiety, or depression, as well as physical effects such as nausea, vomiting, muscle aches, and cramping, among others. Withdrawal symptoms often lead a person to use the substance again.
Implications of the New Diagnostic Criteria
The new diagnostic criteria are likely to reduce the “all or nothing” thinking that has characterized the substance use field. Tolerance and withdrawal remain major clinical symptoms, but they are no longer the deciding factor in whether an individual “has an addiction.” Substance use disorders, including addiction, can occur with all substances listed in Table 1.1 , not just those that are able to produce tolerance and withdrawal. It is also important to understand that substance use disorders do not occur immediately but over time, with repeated misuse and development of more symptoms. This means that it is both possible and highly advisable to identify emerging substance use disorders, and to use evidence-based early interventions to stop the addiction process before the disorder becomes more chronic, complex, and difficult to treat.
What is an Intervention?
Intervention here and throughout this Report means a professionally delivered program, service, or policy designed to prevent substance misuse or treat an individual's substance use disorder. It does not refer to an arranged meeting or confrontation intended to persuade a friend or loved one to quit their substance misuse or enter treatment—the type of “intervention” sometimes depicted on television. Planned surprise confrontations of the latter variety—a model developed in the 1960s, sometimes called the “Johnson Intervention”—have not been demonstrated to be an effective way to engage people in treatment. 68 Confrontational approaches in general, though once the norm even in many behavioral treatment settings, have not been found effective and may backfire by heightening resistance and diminishing self-esteem on the part of the targeted individual. 69
This type of proactive clinical monitoring and management is already done within general health care settings to address other potentially progressive illnesses that are brought about by unhealthy behaviors. 70 For example, patients with high blood pressure may be told to adjust their activity and stress in order to reduce the progression of hypertension. Typically, these individuals are also clinically monitored for key symptoms to ensure that symptoms do not worsen.
See Chapter 6 - Health Care Systems and Substance Use Disorders .
There are compelling reasons to apply similar procedures in emerging cases of substance misuse. Routine screening for alcohol and other substance use should be conducted in primary care settings to identify early symptoms of a substance use disorder (especially among those with known risk and few protective factors). This should be followed by informed clinical guidance on reducing the frequency and amount of substance use, family education to support lifestyle changes, and regular monitoring.
Research has shown that substance use disorders are similar in course, management, and outcome to other chronic illnesses, such as hypertension, diabetes, and asthma. 71 Unfortunately, substance use disorders have not been treated, monitored, or managed like other chronic illnesses, nor has care for these conditions been covered by insurance to the same degree. Nonetheless, it is possible to adopt the same type of chronic care management approach to the treatment of substance use disorders as is now used to manage most other chronic illnesses. 70 - 72 Evidence-based behavioral interventions, medications, social support services, clinical monitoring, and RSS make this type of chronic care management possible, often by the same health care teams that currently treat other chronic illnesses.
See Chapter 4 - Early Intervention , Treatment, and Management of Substance Use Disorders and Chapter 6 - Health Care Systems and Substance Use Disorders .
Evidence also shows that such an approach will improve the effectiveness of treatments for substance use disorders. Remission of substance use and even full recovery can now be achieved if evidence-based care is provided for adequate periods of time, by properly trained health care professionals, and augmented by supportive monitoring, RSS, and social services. This fact is supported by a national survey showing that there are more than 25 million individuals who once had a problem with alcohol or drugs who no longer do. 73
- The Separation of Substance Use Treatment and General Health Care
Until quite recently, substance misuse problems and substance use disorders were viewed as social problems, best managed at the individual and family levels, and sometimes through the existing social infrastructure—such as schools and places of worship, and, when necessary, through civil and criminal justice interventions. 74 In the 1970s, when rates of substance misuse increased, including by college students and Vietnam War veterans, most families and traditional social services were not prepared to handle this problem. 75 Despite a compelling national need for treatment, the existing health care system was neither trained to care for nor especially eager to accept patients with substance use disorders.
For these reasons, a new system of substance use disorder treatment programs was created, but with administration, regulation, and financing placed outside mainstream health care. 74 , 75 This meant that with the exception of detoxification in hospital-based settings, virtually all treatment was delivered by programs that were geographically, financially, culturally, and organizationally separate from mainstream health care. Of equal historical importance was the decision to focus treatment only on addiction. This left few provisions for detecting or intervening clinically with the far more prevalent cases of early-onset, mild, or moderate substance use disorders.
Creating this system of substance use disorder treatment programs was a critical element in addressing the burgeoning substance use disorder problems in our nation. However, that separation also created unintended and enduring impediments to the quality and range of care options. For example, separate systems for substance use disorder treatment and other health care needs may have exacerbated the negative public attitudes toward people with substance use disorders. Additionally, the pharmaceutical industry was hesitant to invest in the development of new medications for individuals with substance use disorders, because they were not convinced that a market for these medications existed. Consequently, until the 1990s, few U.S. Food and Drug Administration (FDA) approved medications were available to treat addictions. 76 , 77
Meanwhile, despite numerous research studies documenting high prevalence rates of substance use disorders among patients in emergency departments, hospitals, and general medical care settings, mainstream health care generally failed to recognize or address substance use disorders. 78 In fact, a recent study by the CDC found that in 2011, only 1 in 6 United States adults and 1 in 4 binge drinkers had ever been asked by a health professional about their drinking behavior. 79 Furthermore, the percent of adult binge drinkers who had been asked about their drinking had not changed since 1997, reflecting the challenges involved in fostering implementation of screening and counseling services for alcohol misuse in clinical settings. This has been a costly mistake, with often deadly consequences. A recent study showed that the presence of a substance use disorder often doubles the odds for the subsequent development of chronic and expensive medical illnesses, such as arthritis, chronic pain, heart disease, stroke, hypertension, diabetes, and asthma. 80
In this regard, fatal medication errors due to unforeseen interactions between a prescribed medication for a diagnosed medical condition and unscreened, unaddressed patient substance use increased ten-fold over the past 20 years. 81 To address this problem, researchers suggested “…(1) screening patients for use…of alcohol and/or street drugs; (2) taking extra precautions when prescribing medicines with known dangerous interactions with alcohol and/or street drugs; and (3) teaching the patient the risks of mixing medicines with alcohol and/or street drugs.” 81 Similar recommendations focusing on prescribed opioids have been issued by the CDC to curb the rise in opioid overdose deaths. 82 Again, screening for substance use and substance use disorders before and during the course of opioid prescribing, combined with patient education, are recommended. 82
Yet despite these and other indications of extreme threats to health care quality, safety, effectiveness, and cost containment, as of this writing, few general health care organizations screen for, or offer services for, the early identification and treatment of substance use disorders. Moreover, few medical, nursing, dental, or pharmacy schools teach their students about substance use disorders; 83 - 86 and, until recently, few insurers offered adequate reimbursement for treatment of substance use disorders. 87 , 88
- Recent Changes in Health Care Policy and Law
The longstanding separation of substance use disorders from the rest of health care began to change with enactment of the Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA) and the Affordable Care Act in 2010. 89 , 90 MHPAEA requires that the financial requirements and treatment limitations imposed by health plans and insurers for substance use disorders be no more restrictive than the financial requirements and treatment limitations they impose for medical and surgical conditions. The Affordable Care Act requires the majority of United States health plans and insurers to offer prevention, screening, brief interventions, and other forms of treatment for substance use disorders. 89
It is difficult to overstate the importance of these two Acts for creating a public health-oriented approach to reducing substance misuse and related disorders. These laws and related changes in health care financing are creating incentives for health care organizations to integrate substance use disorder treatment with general health care. Many questions remain, but those questions are no longer whether but how this much-needed integration will occur. These changes combine to create a new, challenging but exceptionally promising era for the prevention and treatment of substance use disorders and set the context for this Report .
- Marijuana: A Changing Legal and Research Environment
Although this Report does not examine the issue of marijuana legalization, its continually evolving legal status is worth mentioning because of implications for both research and policy. As mentioned elsewhere, marijuana is the most commonly used illicit drug in the United States, with 22.2 million people aged 12 or older using it in the past month. 3 In recent years marijuana use has become more socially acceptable among both adults and youth, while perceptions of risk among adolescents of the drug's harms have been declining over the past 13 years. 91
As use of marijuana and its constituent components and derivatives becomes more widely accepted, it is critical to strengthen understanding of the effects and consequences for individual users and for public health and safety. Conducting such research can be complex as laws and policies vary significantly from state to state. For example, some states use a decriminalization model, which means production and sale of marijuana are still illegal and no legal marijuana farms, distributors, companies, stores, or advertising are permitted. Through ballot initiatives, other states have “legalized” marijuana use, which means they allow the production and sales of marijuana for personal use. Additionally, some states have legalized marijuana for medical purposes, and this group includes a wide variety of different models dictating how therapeutic marijuana is dispensed. The impacts of state laws regarding therapeutic and recreational marijuana are still being evaluated, although the differences make comparisons between states challenging. 92
As of June 2016, 25 states and the District of Columbia have legalized medical marijuana use. Four states have legalized retail sales; the District of Columbia has legalized personal use and home cultivation (both medical and recreational), with more states expecting to do so. None of the permitted uses under state laws alters the status of marijuana and its constituent compounds as illicit drugs under Schedule I of the federal Controlled Substances Act. 93 It should also be noted that use for recreational purposes has not been legalized by any jurisdiction for people under age 21, and few jurisdictions have legalized medical marijuana for young people. While laws are changing, so too is the drug itself with average potency more than doubling over the past decade (1998 to 2008). 94 The ways marijuana is used are also changing - in addition to smoking, consuming edible forms like baked goods and candies, using vaporizing devices, and using high-potency extracts and oils (e.g., “dabbing”) are becoming increasingly common. 95 Because these products and methods are unregulated even in states that have legalized marijuana use, users may not have accurate information about dosage or potency, which can lead and has led to serious consequences such as hospitalizations for psychosis and other overdose-related symptoms. 95 Marijuana use can also impair driving skills and, while estimates vary, is linked to a roughly two-fold increase in accident risk. 96 - 98 The risk is compounded when marijuana is used with alcohol. 96 , 99
There is a growing body of research suggesting the potential therapeutic value of marijuana's constituent cannabinoid chemicals in numerous health conditions including pain, nausea, epilepsy, obesity, wasting disease, addiction, autoimmune disorders, and other conditions. Given the possibilities around therapeutic use, it is necessary to continue to explore ways of easing existing barriers to research. Marijuana has more than 100 constituent cannabinoid compounds, with cannabidiol (CBD) and tetrahydrocannabinol (THC, the chemical responsible for most of marijuana's intoxicating effects) being the most well-studied. Evidence collected so far in clinical investigations of the marijuana plant is still insufficient to meet FDA standards for a finding of safety and efficacy for any therapeutic indications. However, the FDA has approved three medications containing synthetically derived cannabinoids: Marinol capsules and Syndros oral solution (both containing dronabinol, which is identical in chemical structure to THC), and Cesamet capsules (containing nabilone, which is similar in structure to THC) for severe nausea and wasting in certain circumstances, for instance in AIDS patients. Recognizing the potential therapeutic importance of compounds found in marijuana, the FDA has granted Fast Track designation to four development programs of products that contain marijuana constituents or their synthetic equivalents. The therapeutic areas in which products are being developed granted Fast Track by FDA include the treatment of pain in patients with advanced cancer; treatment of Dravet syndrome (two programs), a rare and catastrophic treatment-resistant form of childhood epilepsy; and treatment of neonatal hypoxic ischemic encephalopathy, brain injury resulting from oxygen deprivation during birth.
Additionally, there are clinical investigations for the treatment of refractory seizure syndromes, including Lennox Gastaut Syndrome, and for treatment of post-traumatic stress disorder (PTSD). However, further exploration of these issues always requires consideration of the serious health and safety risks associated with marijuana use. Research shows that risks can include respiratory illnesses, dependence, mental health-related problems, and other issues affecting public health such as impaired driving. Within this context of changing marijuana policies at the state level, research is needed on the impact of different models of legalization and how to minimize harm based on what has been learned from legal substances subject to misuse, such as alcohol and tobacco. Continued assessment of barriers to research and surveillance will help build the best scientific foundation to support good public policy while also protecting the public health.
- Purpose, Focus, and Format of the Report
The Audience
This Report is intended for individuals, families, community members, educators, health care professionals, public health practitioners, advocates, public policymakers, and researchers who are looking for effective, sustainable solutions to the problems created by alcohol and other substances. To meet those needs, the Report reviews and synthesizes the most important and reliable scientific findings in key topic areas and distills those findings into recommendations for:
- Improving public awareness of substance misuse and related problems;
- Reducing negative attitudes related to substance use disorders;
- Closing the gap between what is known to reduce substance misuse at the population level and within specific subgroups, and the implementation of these effective programs, policies, and environmental strategies at the federal, state, and community levels;
- Understanding the need for and effectiveness of programs for high-risk populations;
- Expanding the capacity of health care systems to deliver evidence-based substance use disorder treatment;
- Integrating financing and health care system models to facilitate access and affordability of care for substance use disorders;
- Continuing to build the science base of effective prevention, treatment, and recovery practices and policies; and
- Engaging stakeholders in reducing substance use and misuse problems and protecting the health of all individuals across the lifespan.
Because of the broad audience, the Report is purposely written in accessible language without excessive scientific jargon. The Report also focuses on current issues and practical questions that trouble so many people:
- What are the health and social impacts of alcohol and drug use and misuse in the United States? What key factors influence these behaviors?
- What are the major substance misuse problems facing the United States?
- What causes substance use disorders and why do they change people so dramatically?
- Can substance misuse problems and disorders be prevented? How?
- What constitutes effective treatment?
- Can addicted individuals recover? What will it take to manage their disorders and sustain recovery?
Topics Covered in the Report
Individual chapters in the Report review the science associated with the major substance use, misuse, and disorder issues for specific topics. Tobacco, also an addictive substance, is mentioned only briefly, because problems associated with tobacco use and nicotine addiction have been covered extensively in other Surgeon General's Reports. 14 - 16 , 100 - 103
Because of the broad audience and the practical emphasis, the Report is intentionally selective rather than exhaustive, emphasizing findings that have the potential for the greatest public health impact and the greatest potential for action. For readers wanting greater scientific detail or more specific information, detailed research reports, as well as supplemental resource materials, are supplied in references, in the Appendices, and in special emphasis boxes throughout the Report .
Scientific Standards Used to Develop the Report
Findings cited in all of the chapters came from electronic database searches of research articles published in English. Within those searches, priority was given to systematic literature reviews and to findings that were replicated by multiple controlled trials. However, many important issues in prevention, treatment, recovery, and health care systems have not yet been examined in rigorous controlled trials, or are not appropriate for such research designs. In these cases, the best available evidence was cited and labeled according to the reporting conventions published by the CDC: 104
- Well-supported: Evidence derived from multiple controlled trials or large-scale population studies.
- Supported: Evidence derived from rigorous but fewer or smaller trials or restricted samples.
- Promising: Findings that do not derive from rigorously controlled studies but that nonetheless make practical or clinical sense and are widely practiced.
In cases in which evidence was based on findings of neurobiological research, the CDC standards were adapted.
A summary of the key findings appears at the beginning of each chapter. The key findings highlight what is currently known from available research about the chapter topic, as well as the strength of the evidence. As with the rest of the Report , the key findings are not intended to be exhaustive, but are instead considered the important “take-aways” from each chapter. Readers interested in a fuller discussion of the topics are encouraged to read the chapters in their entirety.
Addressing Substance Use in Specific Populations
As indicated, the chapters are designed to prioritize best available research findings that apply most broadly across different substances and across various subgroups, while also identifying program and policy interventions that have strong evidence for particular substances (e.g., alcohol), when available. The rationale for this decision is that the available research suggests that the genetic, neurobiological, and environmental processes underlying substance use, misuse, and disorders are largely similar across most known substances and unrelated to the age, sex, race and ethnicity, gender identity, or culture of the individual. The available research also clearly indicates that many of the interventions, including population-level policies, focused programs, behavioral therapies, medications, and social services shown to be effective in one subgroup are generally effective for other subgroups. Put differently, it is reasonable to assume that the findings presented in this Report are relevant for many substance use types and patterns; for most age, gender, racial and ethnic, and cultural subgroups; and for many special needs subgroups (e.g., those with co-occurring mental or physical illnesses; those involved with the criminal justice system).
However, this general statement has some important caveats. First, the statement depends heavily on the phrase “available research.” There is insufficient research examining subgroup differences in the neurobiology of substance use disorders and in interventions aimed at preventing, treating, and promoting recovery from substance use disorders. Additional research designed to examine these differences and to test interventions in specific populations is needed.
A second caveat is that individual variability in response to standard prevention, treatment, and recovery support interventions is common throughout health care. Individuals with the same disease often react quite differently to the same medicine or behavioral intervention. Accordingly, general health care has moved toward “personalized medicine,” an individualized treatment regimen derived from specific information about the individual's genetics and stage of illness, as well as lifestyle, language, culture, and personal preferences. Personalized care is not common in the substance use disorder field because many prevention, treatment, and recovery regimens were created as standardized “programs” rather than individualized protocols.
The third caveat to the statement on general research findings is that even if research has shown that certain medications, therapies, or recovery support services are likely to be effective , this does not mean that they will be adequate , especially for groups with specific needs. For example, a medication that is effective in blocking the rewarding effects of opioid use will not fully address the multiple, complex problems of those with opioid use disorders, nor address any co-occurring health conditions such as depression or HIV/AIDS.
Recognizing these limitations to the generalizability of research findings, each chapter has a dedicated section on Specific Populations that focuses particularly on age, racial and ethnic subgroups, and individuals with co-occurring mental and physical illnesses. Findings relevant to other important groups (e.g., military veterans; lesbian, gay, bisexual, and transgender [LGBT] populations; those with criminal justice involvement; those in rural areas) are referred to throughout the Report when available.
The Organization of the Report
This Report is divided into Chapters, highlighting the key issues and most important research findings in those topics. The final chapter concludes with recommendations for key stakeholders, including implications for practice and policy.
This Chapter 1 - Introduction and Overview describes the overall rationale for the Report , defines key terms used throughout the Report , introduces the major issues covered in the topical chapters, and describes the organization, format, and the scientific standards that dictated content and emphasis within the Report .
Chapter 2 - The Neurobiology of Substance Use , Misuse, and Addiction reviews brain research on the neurobiological processes that turn casual substance use into a compulsive disorder.
Chapter 3 - Prevention Program and Policies reviews the scientific evidence on preventing substance misuse, substance use-related problems, and substance use disorders.
Chapter 4 - Early Intervention , Treatment, and Management of Substance Use Disorders describes the goals, settings, and stages of treatment, and reviews the effectiveness of the major components of early intervention and treatment approaches, including behavioral therapies, medications, and social services.
Chapter 5 - Recovery : The Many Paths to Wellness discusses perspectives on remission and recovery from substance use disorders and reviews the types and effectiveness of RSS.
Chapter 6 - Health Care Systems and Substance Use Disorders reviews ongoing changes in organization, delivery, and financing of care for substance use disorders in both specialty treatment programs and in mainstream health care settings.
Chapter 7 - Vision for the Future: A Public Health Approach presents a realistic vision for a comprehensive, effective, and humane public health approach to addressing substance misuse and substance use disorders in our country, including actionable recommendations for parents, families, communities, health care organizations, educators, researchers, and policymakers.
The Appendices provide additional detail about the topics covered in this Report . Appendix A - Review Process for Prevention Programs details the review process for the prevention programs included in Chapter 3 and the evidence on these programs; Appendix B - Evidence-Based Prevention Programs and Policies provides detail on scientific evidence grounding the programs and policies discussed in Chapter 3 ; Appendix C - Resource Guide provides resources specific to those seeking information on preventing and treating substance misuse or substance use disorders; and Appendix D - Important Facts about Alcohol and Drugs contains facts about alcohol and specific drugs, including descriptions, uses and possible health effects, treatment options, and statistics as of 2015.
Moderate alcohol use is defined by the 2015-2020 Dietary Guidelines for Americans as up to 1 drink per day for women and up to 2 drinks per day for men—and only by adults of legal drinking age. Many individuals should not consume alcohol, including individuals who are taking certain over-the-counter or prescription medications or who have certain medical conditions, those who are recovering from an alcohol use disorder or are unable to control the amount they drink, and anyone younger than age 21 years. In addition, drinking during pregnancy may result in negative behavioral or neurological consequences in the offspring.
- Cite this Page Substance Abuse and Mental Health Services Administration (US); Office of the Surgeon General (US). Facing Addiction in America: The Surgeon General's Report on Alcohol, Drugs, and Health [Internet]. Washington (DC): US Department of Health and Human Services; 2016 Nov. CHAPTER 1, INTRODUCTION AND OVERVIEW OF THE REPORT.
- PDF version of this title (12M)
- Disable Glossary Links
In this Page
Other titles in these collections.
- Reports of the Surgeon General
- Health Services/Technology Assessment Texts (HSTAT)
Related information
- PMC PubMed Central citations
- PubMed Links to PubMed
Recent Activity
- INTRODUCTION AND OVERVIEW OF THE REPORT - Facing Addiction in America INTRODUCTION AND OVERVIEW OF THE REPORT - Facing Addiction in America
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers

Here's What a Massive New NIH Addiction Study Found
Community interventions preventing opioid overdoses failed, but don't panic yet..
Posted June 21, 2024 | Reviewed by Tyler Woods
- What Is Addiction?
- Find a therapist to overcome addiction
- A Healing Communities study identified 19 evidence-based recovery strategies to implement in the U.S.
- Follow-up studies should be more positive: 483 deaths were averted in intervention arm, compared to control.
- Until cures are found, long-term methadone treatment with 5-year outcomes need support and reporting.
- Prevention is an underfunded and complementary addiction strategy.
Discouragingly, an ambitious study recently reported in the New England Journal of Medicine did not prove evidence-based interventions like distributing naloxone (Narcan) and providing access to medication -assisted treatments (MATs) significantly curbed opioid deaths. Likely reasons for these findings start with the opioid epidemic as a moving target. False dichotomy either/or thinking is another issue, as both prevention and harm reduction are crucial to saving lives. Trying to end or delay use is also an unacknowledged but viable strategy.

Child and adolescent psychiatrist Sarah Vinson, M.D., Chair, Morehouse School of Medicine’s Department of Psychiatry & Behavioral Sciences, said, “The opioid crisis is driven by many factors that cannot be easily factored into any study, such as despair, poverty, genes , gene expression linked to secondhand drug or trauma exposure, housing, mental illness, involvement in the criminal legal system, other social determinants, and global drug manufacturing, distribution and selling entrepreneurship. Bottom line is primary prevention of drug use is underutilized and very poorly funded.”
Dr. Vinson noted the age of first use of a substance is key. “It is clear substance use disorders starting in 10-year-olds or teens need very different interventions and treatments than SUDs in physician addicts in their 30s.”
Considering the Study
The National Institutes of Health (NIH) awarded $344 million to fund the HEALing Communities study. The focus was on overdose education , naloxone distribution, and medications treating opioid use disorder (OUD). This historic effort, launched in April 2018, was touted to reduce opioid deaths by 40 percent, boost addiction medicine, and create an infrastructure to coordinate responses to OUD.
Sadly, the study found rates of opioid-related overdose deaths did not differ compared to the control group. However, much was learned in this program implementing evidence-based treatment approaches, coalitions, and health system delivery building. While the headline now is failure of harm reduction, the data will continue to be evaluated, interventions modified/eliminated, and more positive findings reported. Still, I think longer-term implementation could have created better results.
Reflections on Study Outcomes and What Works
Naloxone distribution and encouraging medication-assisted treatments are life-saving. They are often the last resort compared to prevention or interventions. Said National Institute on Drug Abuse (NIDA) director Nora Volkow, M.D., “This study brought researchers, providers, and communities together to break down barriers and promote the use of evidence-based strategies that we know are effective.” She added, “It’s clear we need to continue developing new tools and approaches for addressing the overdose crisis…”
Possible Reasons for Study Outcomes
Why did communities implementing public health strategies not see a statistically significant reduction in opioid overdose deaths?
The opioid overdose crisis: A moving target. The opioid crisis is a moving target, quickly making public health approaches obsolete. For example, counterfeit fentanyl-containing pills and heroin, cocaine, and methamphetamine, as well as xylazine combined with lab-made fentanyl, escalated death rates. Consequently, a death rescue strategy built for heroin overdoses, with patients treated with low doses of naloxone delivered intranasally in the community, was behind the curve once fentanyl dominated the former heroin user market. Fentanyl is uniquely dangerous, addicting, and anhedonia -inducing alone, challenging harm-reduction efforts.
Harm reduction doesn’t equal prevention or cure. Addiction is a chronic, relapsing, long-term disease, often ending with premature death. Harm reduction is important but not a cure, as more than 20 percent of all opioid overdose decedents received naloxone but died anyway. NIDA has funded new treatment development and research on overdose, psychedelics, brain neuromodulation, neurosurgery , immunological treatment, and vaccines . Focusing on at least five years of methadone treatment makes harm reduction and treatment sense.
Looking back. When tobacco use peaked in the mid-1960s, more than 40 percent of adults in the U.S. smoked cigarettes. Stigmatizing cigarette smokers was an important means of ending the tobacco epidemic. The tobacco smoking epidemic was reversed not by new treatments for nicotine use disorders, but public anti-smoking campaigns, legislation, and hefty taxation. Anti-tobacco campaigns made tobacco dangerous and changed social norms.
Imagine if the tobacco harm reduction approach had persisted. In that case, we might still have tobacco addiction deniers, smoking at work and in restaurants, and cheap cigarettes everywhere.
We must reduce stigma to get folks into treatment and ensure they aren’t ostracized. Inadvertently, we stopped raising the alarm about the dangers of drugs when what we need to do is stigmatize the drugs themselves .

An either-or dichotomy: MATs or prevention. Billions of federal dollars have been spent saving many lives from overdose. The current fentanyl death crisis is a speedballing and poly -drug zombie era. Nowadays, prevention is unrelated to stopping physicians from writing too many opioid prescriptions. We need new prevention ideas, targets, and tactics. I remember Dr. Dave Smith’s terse but effective motto: “Speed Kills,” and the anti-use impact of Len Bias ’s and John Belushi’s deaths.
With support, Anne Milgram’s “One Pill Can Kill” could be an effective preventive message. Programs like the Office of National Drug Control Policy’s Drug-Free Communities, which have proven success reducing youth substance use, should be part of community evidence-based solutions.
There has been almost no new investment in stopping or delaying drug use in the first place—the most cost-effective way to reduce the number of new people entering pathways leading to overdose and death.
Many teens today choose not to use alcohol , cannabis, and other drugs. We need to support teens with prevention initiatives, in addition to providing overdose reversal, MAT treatment, and years-long continuation of addiction treatment.
We have decades of experience evaluating and treating physicians and other health providers with OUDs and SUDs. At the five-year follow-up, 80 percent of these resource-rich patients are in recovery and at work. I wish such treatment were available to everyone who wanted it.

In his book The New Addiction Treatment , David Patterson Silver Wolf reported patients refusing treatment and others repeatedly treated with the same treatment. In his paper , relapsing OUD was blamed on the patient—rather than the limited treatments available.
While not finding the reduced deaths expected, this harm reduction study facilitated remarkable community engagement, best practices and treatment system building. More good news from the study will likely come in the future. Strategies focusing exclusively on people already using drugs—rather than also investing in stopping or delaying use among youth and young adults—may explain the ever-changing continuous drug death tragedy in the U.S.
HEALing Communities Study Consortium; Samet JH, et. Al. Community-Based Cluster-Randomized Trial to Reduce Opioid Overdose Deaths. N Engl J Med. 2024 Jun 16. doi: 10.1056/NEJMoa2401177. Epub ahead of print. PMID: 38884347.
Kosten TR. Vaccines as Immunotherapies for Substance Use Disorders. Am J Psychiatry. 2024 May 1;181(5):362-371. doi: 10.1176/appi.ajp.20230828. PMID: 38706331.
DuPont RL, McLellan AT, White WL, Merlo LJ, Gold MS. Setting the standard for recovery: Physicians' Health Programs. J Subst Abuse Treat. 2009 Mar;36(2):159-71. doi: 10.1016/j.jsat.2008.01.004. PMID: 19161896.
Patterson Silver Wolf DA, Gold M. Treatment resistant opioid use disorder (TROUD): Definition, rationale, and recommendations. J Neurol Sci. 2020 Apr 15;411:116718. doi: 10.1016/j.jns.2020.116718. Epub 2020 Feb 5. PMID: 32078842.

Mark S. Gold, M.D., is a pioneering researcher, professor, and chairman of psychiatry at Yale, the University of Florida, and Washington University in St Louis. His theories have changed the field, stimulated additional research, and led to new understanding and treatments for opioid use disorders, cocaine use disorders, overeating, smoking, and depression.
- Find a Therapist
- Find a Treatment Center
- Find a Psychiatrist
- Find a Support Group
- Find Online Therapy
- United States
- Brooklyn, NY
- Chicago, IL
- Houston, TX
- Los Angeles, CA
- New York, NY
- Portland, OR
- San Diego, CA
- San Francisco, CA
- Seattle, WA
- Washington, DC
- Asperger's
- Bipolar Disorder
- Chronic Pain
- Eating Disorders
- Passive Aggression
- Personality
- Goal Setting
- Positive Psychology
- Stopping Smoking
- Low Sexual Desire
- Relationships
- Child Development
- Self Tests NEW
- Therapy Center
- Diagnosis Dictionary
- Types of Therapy

At any moment, someone’s aggravating behavior or our own bad luck can set us off on an emotional spiral that could derail our entire day. Here’s how we can face triggers with less reactivity and get on with our lives.
- Emotional Intelligence
- Gaslighting
- Affective Forecasting
- Neuroscience
Int’l Day Against Drug Abuse
Experts for implementing steps to effectively deal with challenge of drug addiction RECORDER REPORT ISLAMABAD: Health experts Wednesday urged the government to address issue of cigarette smoking and implement robust fiscal/regulatory measures to ultimately prevent drug addiction on the occasion of International Day Against Drug Abuse 2024. This message has been given by a group of experts during an event held here on Tuesday in connection with the International Day Against Drug Abuse 2024. The day is dedicated to raising awareness about the dangers of drug abuse and promoting a drug-free society. The theme for 2024, “Prevention is Better” underscores the importance of preventive measures in combating the global drug problem. This year, the focus is on the critical role of early intervention and education in preventing substance abuse, with particular attention to the role of cigarettes as a gateway to more dangerous drugs. Experts said the first step towards drug abuse research has consistently shown that cigarette smoking often serves as the first step towards the use of more harmful substances. Nicotine addiction, which develops through cigarette smoking, can lead individuals to seek stronger and more addictive substances. The progression from cigarettes to drugs like marijuana, cocaine, and other illicit substances is a well-documented pathway. This underscores the importance of targeting tobacco use in efforts to prevent drug abuse. In the 2024 budget, the government made a controversial decision by not increasing the Federal Excise Duty (FED) on tobacco products. Additionally, the government increased the pricing threshold, which has provided more leverage for big tobacco companies to maximize their profits. This move has been criticized by public health advocates, who argue that it undermines efforts to reduce smoking rates and, by extension, drug abuse. The decision to keep FED unchanged and to adjust the pricing threshold is seen as a boon for tobacco companies at the expense of public health. Higher taxes on tobacco products are a proven strategy to reduce smoking rates, particularly among youth and low-income populations. By failing to implement such measures, the government is missing a critical opportunity to deter smoking initiation and progression to other forms of substance abuse, they added.
More from the page
Meeting assesses steps to address heat wave issue, specific clauses of ssa between mnt halan pak b v, advans s a sicar, hospital pharmacies, ‘fpcci, senate budget proposals deserve serious consideration’, enhancing exports a must for sustainable growth: senate chief, 25-30pc st on essential healthcare products assailed.

COMMENTS
85 percent of the world's research on drug abuse and addiction. Other sponsoring agencies include the National Institute of Mental Health (NIMH), the National Institute on Alcohol Abuse and Alcoholism (NIAAA), and the Substance Abuse and Mental Health Services Administration (SAMHSA), all in the Department of Health and Human Services; as well as the Office of Justice Programs (OJP) in the ...
Drug use is one of the nation's most expensive health problems, costing $109.8 billion in 1995 alone (Harwood, Fountain, and Livermore, 1998). In addition to the financial costs, drug use also exacts a human cost with thousands of lives being damaged and forever changed by drug use and addiction. Prevention and treatment research, as well as clinical experience, have shown that it is often ...
The numbers for substance use disorders are large, and we need to pay attention to them. Data from the 2018 National Survey on Drug Use and Health suggest that, over the preceding year, 20.3 million people age 12 or older had substance use disorders, and 14.8 million of these cases were attributed to alcohol.When considering other substances, the report estimated that 4.4 million individuals ...
employ comprehensive research, treatment, and policy reforms, as we do with other chronic illnesses such as diabetes, HIV/AIDS, and cancer. In 2016, the U.S. surgeon general released the first-ever "Facing Addiction in America: Surgeon General's Report on Alcohol, Drugs, and Health," which specifically called attention to the
Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition) Published in 2014, this report offered health professionals and other stakeholders information on principles of effective drug addiction treatment, answers to frequently asked questions, an overview of the drug addiction treatment landscape in the United States, and ...
Drug addiction is responsible for millions of deaths per year around the world. Still, its management as a chronic disease is shadowed by misconceptions from the general public. Indeed, drug ...
Findings: For a better understanding of the results, it was deemed advisable to categorize them into: (a) the types of major interventions and the theoretical approaches on which they were based, (b) the results of the review articles according to (1) variables and factors concerning the prevention proved important through the review and (2) a number of more general important topics which ...
Scientists study the effects drugs have on the brain and behavior. They use this information to develop programs for preventing drug use and for helping people recover from addiction. Further research helps transfer these ideas into practice in the community. The consequences of drug use are vast and varied and affect people of all ages.
This Special Collection on Addiction focuses on scientific advances in the treatment and recovery mechanisms of addiction related to four widely misused substances: alcohol, nicotine, cocaine, and opioids. Although the opioid crisis has taken center stage across public policy and scientific forums, all of these substances continue to have a profound global impact on health and well-being and ...
effects of long-term drug abuse throughout the body. For example, research has shown that tobacco smoke causes cancer of the mouth, throat, larynx, blood, lungs, stomach, pancreas, kidney, bladder, and cervix.19 In addition, some drugs of abuse, such as inhalants, are toxic to nerve cells and may damage or destroy them.
1.3 Release of endocannabinoids by abused drugs. The endocannabinoid system can modulate the primary rewarding effects of non-cannabinoid drugs of abuse, and this ability appears to depend on endocannabinoid release in the VTA (Lupica and Riegel 2005).This hypothesis is consistent with evidence that repeated non-contingent drug administration alters levels of the endocannabinoids anandamide ...
The current paper highlights the causes of drug abuse, and describes the treatment and prevention of drug abuse and addiction for proper management of the problem. Discover the world's research 25 ...
The articles in this special issue of Professional Psychology: Research and Practice feature a diverse and equally important collection of psychology's professional contributions, both nationally and internationally, in substance use disorder and addiction research and clinical practice. Articles in this special issue illuminate the relationships between culture and substance use disorder ...
I. Introduction. The United States is currently in the midst of a public health crisis. For the past two decades, the growing opioid crisis, characterized by a skyrocketing level of overdose deaths, has spread throughout the country. In 2017 alone, 47,600 people in the United States died from an opioid overdose, making accidental overdose more ...
The focus on design and methodology as it influences drug use/abuse research stems from my own long-standing professional interests in studies of drug etiology (Scheier, 2010) and prevention (Scheier, 2015). However, there is more to that story as well.
Understandings of drug addiction recovery are still being debated. ... we focused on people with a history of illicit drug addiction because research on this subject is scarce compared to studies on alcohol addiction. ... Galvani S., Clayson A. (2022). Recovery as long term: An introduction. In Long-term recovery from substance use (pp. 3-14 ...
Abstract. The current opioid epidemic is one of the most severe public health crisis in US history. Responding to it has been difficult due to its rapidly changing nature and the severity of its associated outcomes. This review examines the origin and evolution of the crisis, the pharmacological properties of opioids, the neurobiology of opioid ...
Theoretical issues underlying drug abuse are discussed in detail. The paper indicates thaI the youth gels involved in drugs due to peer pressure, curiosity, wanting to be different, rioting from ...
Drug Addiction Research Paper Introduction - Free download as PDF File (.pdf), Text File (.txt) or read online for free. Writing a thesis on drug addiction poses many challenges, as it requires extensive research on a complex topic with multifaceted causes and consequences. Navigating the vast literature from different disciplines, formulating a clear thesis statement that captures the ...
Michigan 48109-1109; e-mail: [email protected], [email protected]. Key W ords sensitization, learning, nucleus accumbens, dopamine, drug abuse. Abstract The development of addiction involves a ...
At the National Institute on Drug Abuse (NIDA), we believe that increased understanding of the basics of addiction will empower people to make informed choices in their own lives, adopt science-based policies and programs that reduce drug use and addiction in their communities, and support scientific research that improves the Nation's well ...
The United States has a serious substance misuse problem. Substance misuse is the use of alcohol or drugs in a manner, situation, amount, or frequency that could cause harm to the user or to those around them. Alcohol and drug misuse and related substance use disorders affect millions of Americans and impose enormous costs on our society. In 2015, 66.7 million people in the United States ...
Key points. A Healing Communities study identified 19 evidence-based recovery strategies to implement in the U.S. Follow-up studies should be more positive: 483 deaths were averted in intervention ...
Experts said the first step towards drug abuse research has consistently shown that cigarette smoking often serves as the first step towards the use of more harmful substances. Nicotine addiction, which develops through cigarette smoking, can lead individuals to seek stronger and more addictive substances.